
Natural killer cell-mediated ADCC in SARS-CoV-2-infected individuals and vaccine recipients
ANTIBODY DEPENDENT EVERYTHIIIIIIIIIIING !

When it rains, it pours…
Natural killer cell-mediated ADCC in SARS-CoV-2-infected individuals and vaccine recipients
Abstract
COVID-19, caused by SARS-CoV-2, has emerged as a global pandemic. While immune responses of the adaptive immune system have been in the focus of research, the role of NK cells in COVID-19 remains less well understood. Here, we characterized NK cell-mediated SARS-CoV-2 antibody-dependent cellular cytotoxicity (ADCC) against SARS-CoV-2 spike-1 (S1) and nucleocapsid (NC) protein. Serum samples from SARS-CoV-2 resolvers induced significant CD107a-expression by NK cells in response to S1 and NC, while serum samples from SARS-CoV-2-negative individuals did not. Furthermore, serum samples from individuals that received the BNT162b2 vaccine induced strong CD107a expression by NK cells that increased with the second vaccination and was significantly higher than observed in infected individuals. As expected, vaccine-induced responses were only directed against S1 and not against NC protein. S1-specific CD107a responses by NK cells were significantly correlated to NK cell-mediated killing of S1-expressing cells. Interestingly, screening of serum samples collected prior to the COVID-19 pandemic identified two individuals with cross-reactive antibodies against SARS-CoV-2 S1, which also induced degranulation of NK cells. Taken together, these data demonstrate that antibodies induced by SARS-CoV-2 infection and anti-SARS-CoV-2 vaccines can trigger significant NK cell-mediated ADCC activity, and identify some cross-reactive ADCC-activity against SARS-CoV-2 by endemic coronavirus-specific antibodies.
Another day, another antibody-mediated mechanism involving SARS-CoV-2 and its Frankenstein protein, this is another form of ADE, in case the reader is lost in the science speak. We have a lot to understand here and unpack. First, what is Antibody-Dependent Cellular Cytotoxicity (ADCC) ? A type of immune reaction in which a target cell or microbe is coated with antibodies and killed by certain types of white blood cells. The white blood cells bind to the antibodies and release substances that kill the target cells or microbes.
In this case, such response was found against both the S1 part of the Spike Protein, and the Nucleocapsid (N) Protein, measured by CD107a. This is a protein that is a marker for the degranulation of specific cells (NK especially). Degranulation is a fancy term for a cell release enzymes to “kill” infected cells, such an enzyme I have mentioned recently, perforin, which literally pokes roles in cell membranes. Before going deeper, you should REALLY read this post, these papers are starting to link everything together.

What is interesting is that they found that vaccinated individuals had much more 107a, than infected individuals, and this response was solely aimed at the S1 part.
For clarity's sake, CD16 is the same as FcγRIII (FC gamma Receptor). And lyse is a term for destroying the outer membrane of cells.
During ADCC, virus-specific antibodies bind to viral antigens present on the surface of infected cells, and recruit cytotoxic effector cells, in particular NK cells, through their CD16 receptor (FcγIII-Receptor) [13]. CD16-mediated activation of NK cells results in degranulation with the release of cytotoxic molecules such as perforin and granzyme [14, 15]. Antiviral activity mediated by ADCC has been described for several viral infections, including HIV-1, influenza, and Ebola [16-18]. Furthermore, studies using the rhesus macaque model for SIV infection have shown that antibody-mediated protection is reduced when the Fc-fraction of neutralizing antibodies is cleaved [19], suggesting that Fc-mediated antiviral activity is an important additional effector function of antibodies.
Results
Antibodies induced by COVID-19 can trigger CD16-mediated NK cell responses
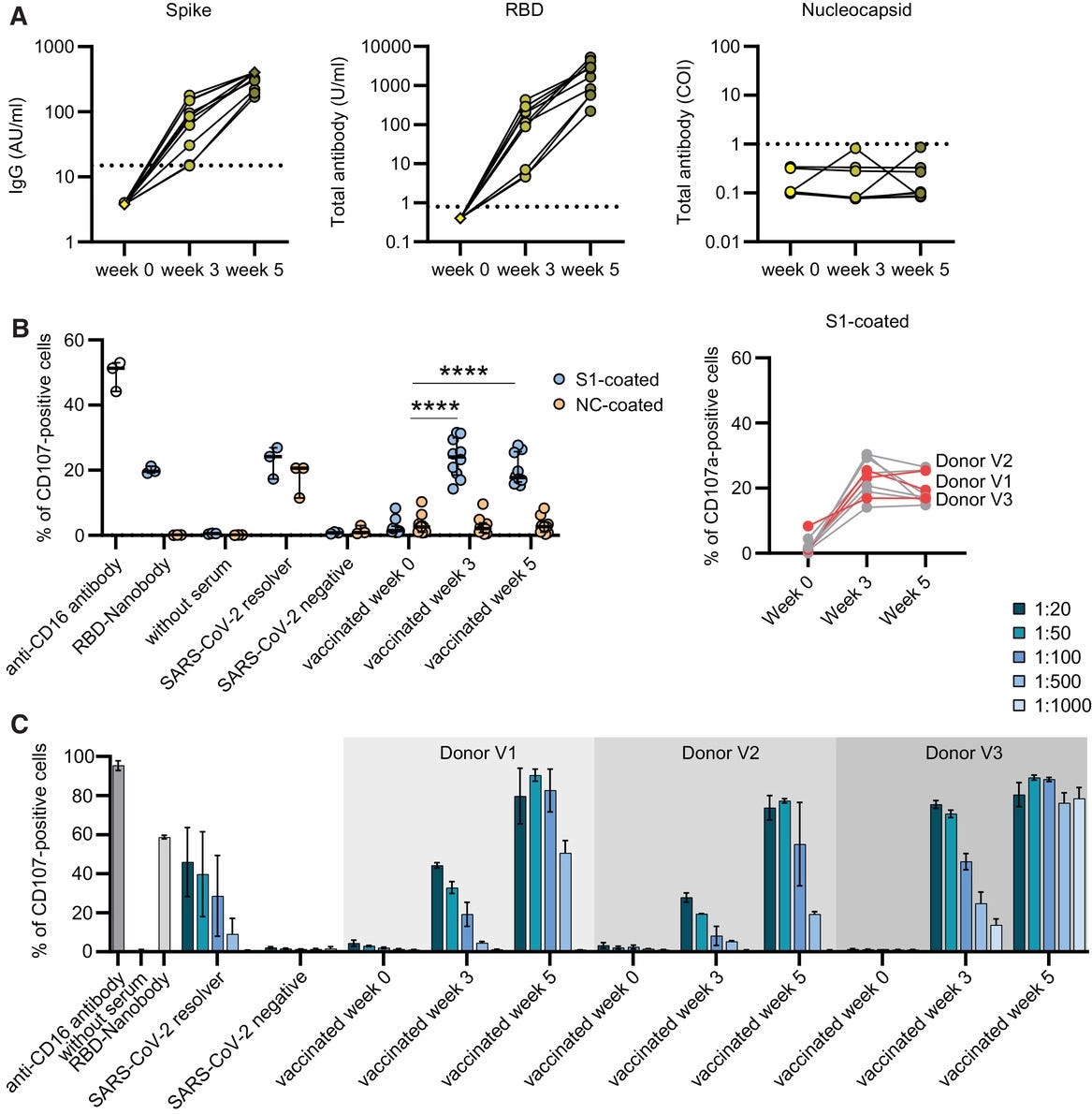
NK cells can lyse virus-infected cells by ADCC mediated by the FcγIII-Receptor, also known as CD16, upon binding to the Fc-part of IgG antibodies [13]. Here, we established a degranulation assay that uses CD107a, a sensitive marker of NK cell degranulation [25], to measure CD16-mediated NK-cell activation. Serum samples of PCR-confirmed SARS-CoV-2 resolvers were screened for specific antibodies against the SARS-CoV-2 S1/S2 spike (n = 15) and nucleocapsid (NC) protein (14 out of 15 tested), and as expected, significantly higher antibody titers were detected in these COVID-19 resolvers compared to healthy control individuals (n = 15)
First paragraph they explain what ADCC is, and diseases that are known to use this mechanism, with my previous explanation of the scientific terms, it is easier to understand. In simple terms, it means that your immune response, especially your antibodies binding to cells, and signaling your immune system with specific receptors, activates NK cells, and they go on to kill that cell. When that occurs, in my opinion, the dead cell release too much “cellular rust, and trash” (ROS, oxidation), and other inflammatory enzymes/proteins, which sets off a continuous stream of low-grade inflammatory response.
The second paragraph and a decent portion of the paper go to show how they found it, and how they measured it. And about healthy controls, and some rare cases of people infected “prior to the pandemic”. But the next part stands out for multiple reasons.
BNT162b2 vaccination induces highly functional antibodies that mediated strong NK cell activation
As expected, NK cell degranulation was only observed in response to S1 protein, while NC protein-directed ADCC responses remained low. Interestingly, while S1-specific antibody titers induced by vaccination continued to increase from weeks 3 to 5 (Fig. 3A), serum-mediated CD107a expression on NK cells remained stable
These additional experiments demonstrated that serum samples from BNT162b2-vaccinated individuals diluted up to 1:500 and for one donor even up to 1:1000 continued to trigger strong NK cell degranulation at week 5. These BNT162b2-induced ADCC responses exceeded those observed in individuals that had been infected with SARS-CoV-2, in which CD107a expression levels by NK cells started to decrease with increasing serum sample dilution. Overall, CD107a expression levels by NK cells using 1:100 diluted serums were significantly correlated to S1 antibody titers
Taken together, these data demonstrate that the BNT162b2 vaccine can induce highly functional antibodies against the SARS-CoV-2 S1 protein that can mediate strong NK cell activation even at dilutions at which reduction of NK cell activation is observed for antibodies induced by natural SARS-CoV-2 infection.
This entire section of the paper is amazing, for multiple reasons. The Natural Killer degranulation, in vaccinated individuals, was found in response to only the S1 part, and minimal to the N protein, this is further evidence that the vaccinated individuals can’t build an immune response (and memory) towards the N protein, which I covered the importance all over here, and in the Reverse Marek posts. If you did read the post I linked above, you are now aware this uses the mechanism of opsonization, meaning covering a cell in antibodies.
Even when diluting the samples, they will found significant CD107a, and it was significantly correlated with the amount of S1 antibodies.
Here, we show strong ADCC activity of antibodies induced by natural SARS-CoV-2 infection that was even stronger for antibodies induced by the BNT162b2 vaccine.
NK cell activation by SARS-CoV-2-directed antibodies resulted in NK cell-mediated lysis of antigen-expressing cells. Taken together, these data demonstrate that antibodies directed against SARS-CoV-2 can induce NK cell-mediated ADCC activity, and that antibodies induced by the BNT162b2 vaccine mediate significantly stronger functional activity of NK cells.
Remarkably, vaccine-induced antibodies mediated significantly stronger ADCC activity at low concentrations compared to antibodies induced by natural SARS-CoV-2 infection, providing an additional correlate for the strong protective effect observed by SARS-CoV-2 vaccines in vivo. While this study focuses on ADCC mediated by RBD-specific antibodies, it has been shown that COVID-19 resolver can also develop high titers of NC-specific antibodies. However, their functional relevance is still controversially discussed, as there is a lack of knowledge regarding host interactions with NC itself. A recent study reported that NC-specific antibodies play an important role in inhibiting complement hyperactivation, resulting in better disease outcome
Outside the science talk, they just discuss what we previously discussed in this analysis. The second paragraph holds much value, since by the fact that the vaccine induces that mediated antibody mechanism much stronger than natural infection. Why would that be a problem, even if we take into consideration just this paper?
Simple. This will occur in ANY cell that gets covered by the antibodies, would not be a problem if the Spike protein from the vaccine was created in a targeted manner, and not systemically. In my opinion, with some evidence presented before, this happens in every breakthrough and would explain why some people have such weird “after effects” after infections, specially recently. Even if Omicron is clinically mild, the after-effects of infections might not be.
The last paragraph is interesting because I think the difference between beneficial or detrimental Nucleocapsid response is… timing of the infection, and how much viral replication occurred. Early, it’s good, later, not so much, but the fact is, an N protein response is necessary and very important to clear the infection. In the post below, there is an entire paragraph about the diverse roles of the immune response towards the N protein.
I will again reiterate my previous… let us call it, insight, or idea, now perhaps the outlines of a hypothesis. The receptor used, and the type of cell that mediates the cell death, dictates what type of cell death that infected cell suffers. T lymphocytes will end up with a specific type of cell death (apoptosis), other ferroptosis, and so on.
I know many vaccinated people get desperate, so here, besides my pinned post, is another thing that will be extremely beneficial in helping you recover. Fasting. In fact, fasting for a few days should be prescribed to any vaccinated individuals today.
Prolonged Fasting Reduces IGF-1/PKA to Promote Hematopoietic-Stem-Cell-Based Regeneration and Reverse Immunosuppression
•Prolonged fasting downregulates a IGF-1/PKA pathway in stem cells
•Prolong fasting protects hematopoietic cells from chemotoxicity
•Prolonged fasting cycles promote HSC self-renewal to reverse immunosuppression
•Inhibition of IGF-1 or PKA signaling mimics the effects of prolonged fasting
See my post about ketones for an even deeper understanding of this. With this out of the way, into a tangential rabbit hole, we go.
NK Cells Activated through Antibody-Dependent Cell Cytotoxicity and Armed with Degranulation/IFN-γ Production Suppress Antibody-dependent Enhancement of Dengue Viral Infection

If you read my Reverse AIDS hypothesis, you will be aware that, for the longest time, I held the view that Interferon-gamma was being expressed at high levels in the vaccinated solely based on the spike protein. But perhaps the spike itself is not the sole target, but it is the body attempting to hold the inflammation. Again, this is just a side thought I decided to write here.
As a final note, this mechanism, ADCC, has specific cell depleting capabilities.
Antibody-dependent fragmentation is a newly identified mechanism of cell killing in vivo
The prevailing view is that therapeutic antibodies deplete cells through opsonization and subsequent phagocytosis, complement-dependent lysis or antibody-dependent cellular-cytotoxicity. We used high resolution in vivo imaging to identify a new antibody-dependent cell death pathway where Kupffer cells ripped large fragments off crawling antibody-coated iNKT cells. This antibody-dependent fragmentation process resulted in lethality and depletion of crawling iNKT cells in the liver sinusoids and lung capillaries. iNKT cell depletion was Fcy-receptor dependent and required iNKT cell crawling. Blood, spleen or joint iNKT cells that did not crawl were not depleted. The antibody required high glycosylation for sufficiently strong binding of the iNKT cells to the Fc Receptors on Kupffer cells. Using an acetaminophen overdose model, this approach functionally depleted hepatic iNKT cells and affected the severity of liver injury. This study reveals a new mechanism of antibody-dependent killing in vivo and raises implications for the design of new antibodies for cancer and auto-reactive immune cells.
Overall we now have a sizable amount of evidence on SARS-CoV-2 mediated ADE in various forms, and the groundwork for the (weird) inflammation, immune dysfunction, and all the subsequential damage. We are inching ever closer to better answers.
You can buy me a coffee whenever you feel like it.
Deep appreciation for all the supporters!
Wow, thank you! I may have actually understood this post, which is a minor miracle. To confirm, there is risk of ADE from both natural infection and also vaccination but the risk is far greater in vaccinated populations?
I will share your post about mitigating the damages of vaccination with several vaccinated friends, thank you!
I haven't read all of your work yet. What do you think of the idea that if bird flu makes the jump to humans we're all screwed? They just culled 150k ducks in Canada due to bird flu "caused by climate change" to go with the 10s of millions of chickens they've culled here in the US. Seems like they're more worried about it this time around.