

Quite a few things to analyze today, first the bad news for some, given how extensive my Galectin substack is (there are over 45 papers in the draft alone), I am pushing it to the next few days, I want to do it properly. Second, I rather dislike uninformative posts, so often I rather not publish anything, rather than publish something ultra-short.
Here is a super-small Twitter thread talking about a recent paper on Long Covid and the increased molecules they found in the blood of the patient in the study. The tweet below this one is where I connect it to the broader picture.


The following paper often sounds like a vaccine sales pitch, which is mostly the norm these days, for either being published or getting funded, but there are many important aspects raised by the authors that they low-key left for the reader to pick up. I will remind you of the importance of these and how they fit into the overall observations I have been writing about after.
This is in line (via different dynamics) with the following one.

Before we delve into what they wrote, be aware that a hallmark of older immune systems is a fairly different immune response.
In this paper, the authors analyzed the immune response of older patients (70+ years) with 2 doses of AstraZeneca, and a booster dose of mRNA vaccine. In line with previous evidence, the B-Cells (antibody-producing cells) had a less neutralizing potency and breadth after the mRNA booster in the elderly in this study, associated with higher levels of atypical B cells.
Atypical B-cells are a subtype of B-cells that are often linked to both old age and vaccination, they have very different kinetic (behavior) in our bodies, and they are often followed by more inflammatory responses.
Not only these cells were more present in the elderly here, but they had poorer expression of Interferon Gamma (one of the main tools to deal with infection), and Interleukin-2. And the T Cell response was impaired.
An interesting observation and an increasing trend among many researchers lately was the use of machine learning to analyze their data. In which they describe with more molecular details which type of B cell, markers for said cells. FcRL5 and CD11c are one of the most commonly used ways to measure the presence of these “atypical” often memory B cells.
The red highlight is the most interesting observation so far, because the authors found that even with high levels of B cells and IgG there was a significant negative correlation between these “atypical” cells and neutralizing capacity.
This is here merely as an observation of points I have made beforehand. Myeloid cells are cells made from Hematopoietic Stem Cells, and the mRNA has an enhanced activation of said cells. This is not merely antigen being presented by the immune system…
To not make things more complex than should be, I found it fascinating that atypical B cells are “created” from your body producing IL-21 and IFN gamma, both inflammatory, both more expressed when you get older, or your immune system age. Both of these lead to an imbalance in the immune system. Ending up in Th17.
The last highlight. We need to go through another paper before I make my point.
Growing research interest in many scientific fields, and of particular interest in regard to SARS-CoV-2 is senescence, in simple terms the loss of the power of your cells, that among many interconnecting dynamics, comes with age (or…inflammation…).
In line with previous findings of other authors, and using different measurements than the authors of the first paper here, authors found that older adults had a diminished T cell response towards the virus, and in older adults the T Cells that respond had a preference to the S2 region of the Spike protein, which is highly conserved, fancy words for “doesn’t mutate tons, is the same in different variants/strains”.
Of particular interest is that this response was not present under the natural infection, which was broad and “normal”.
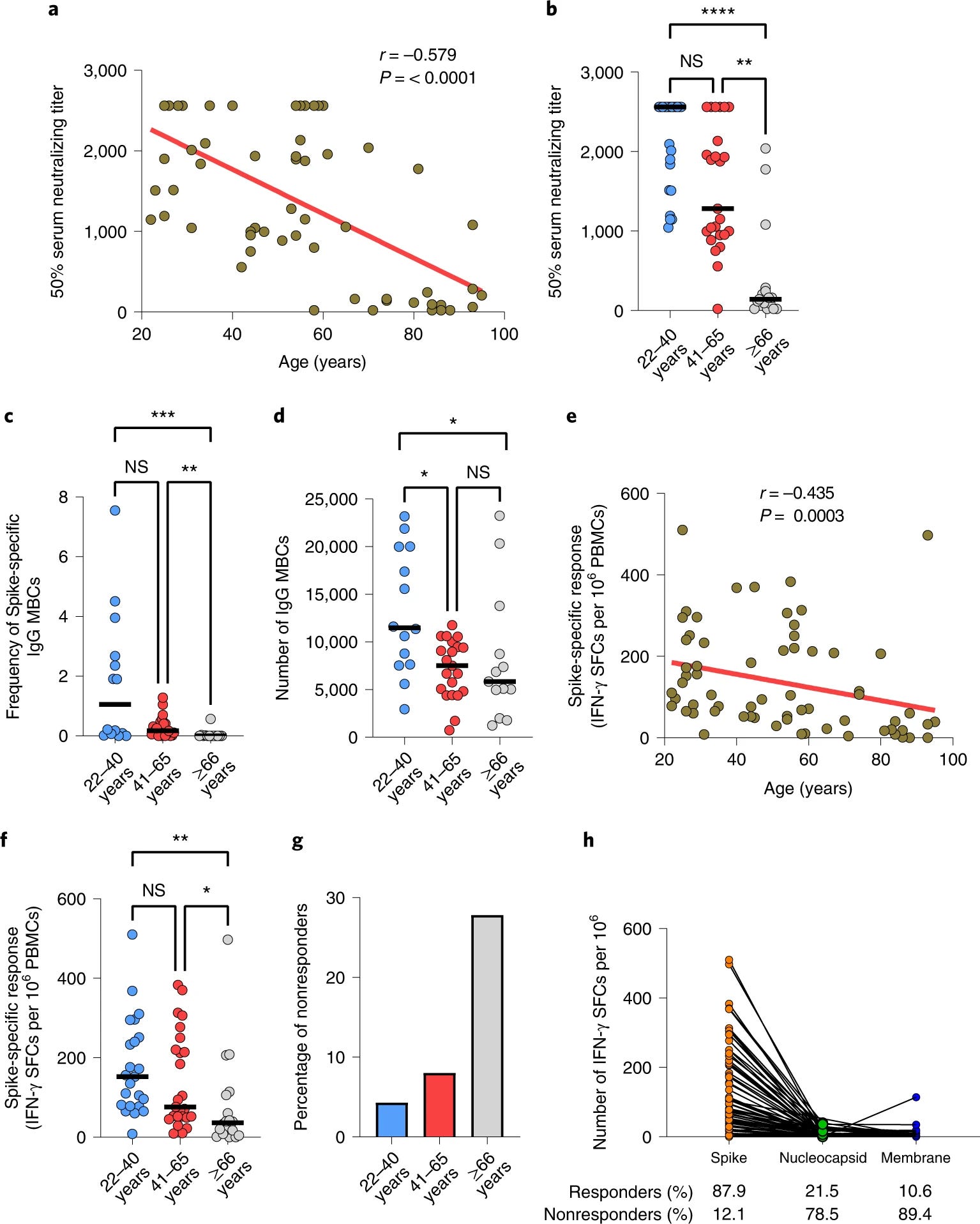
In line with over 18 months of evidence, and many of my earlier observations published here, vaccinated people had a poor conversion (acquiring immunity towards) both the Nucleocapsid (N) and Membrane (M), what is interesting is that these numbers are inversely correlated with age too, so the older the person was, the less immunity towards N and M that person had.
By measuring different markers to further elucidated what the probable mechanism is, they found it is related to senescence, and it is fairly similar to certain chronic infections. Chronic infections, senescence, and inflammanging not only share commonalities but are all parts of the same “thing”, low-grade long-term inflammation leading to improper function of the immune system.
The mRNA vaccine in older adults led to lower frequency of polyfunctional T cells, and “lower quantities” of them. A polyfunctional T cell is a T cell that is able to produce various types of cytokines, less polyfuction = less ability to fight and clear infection properly.
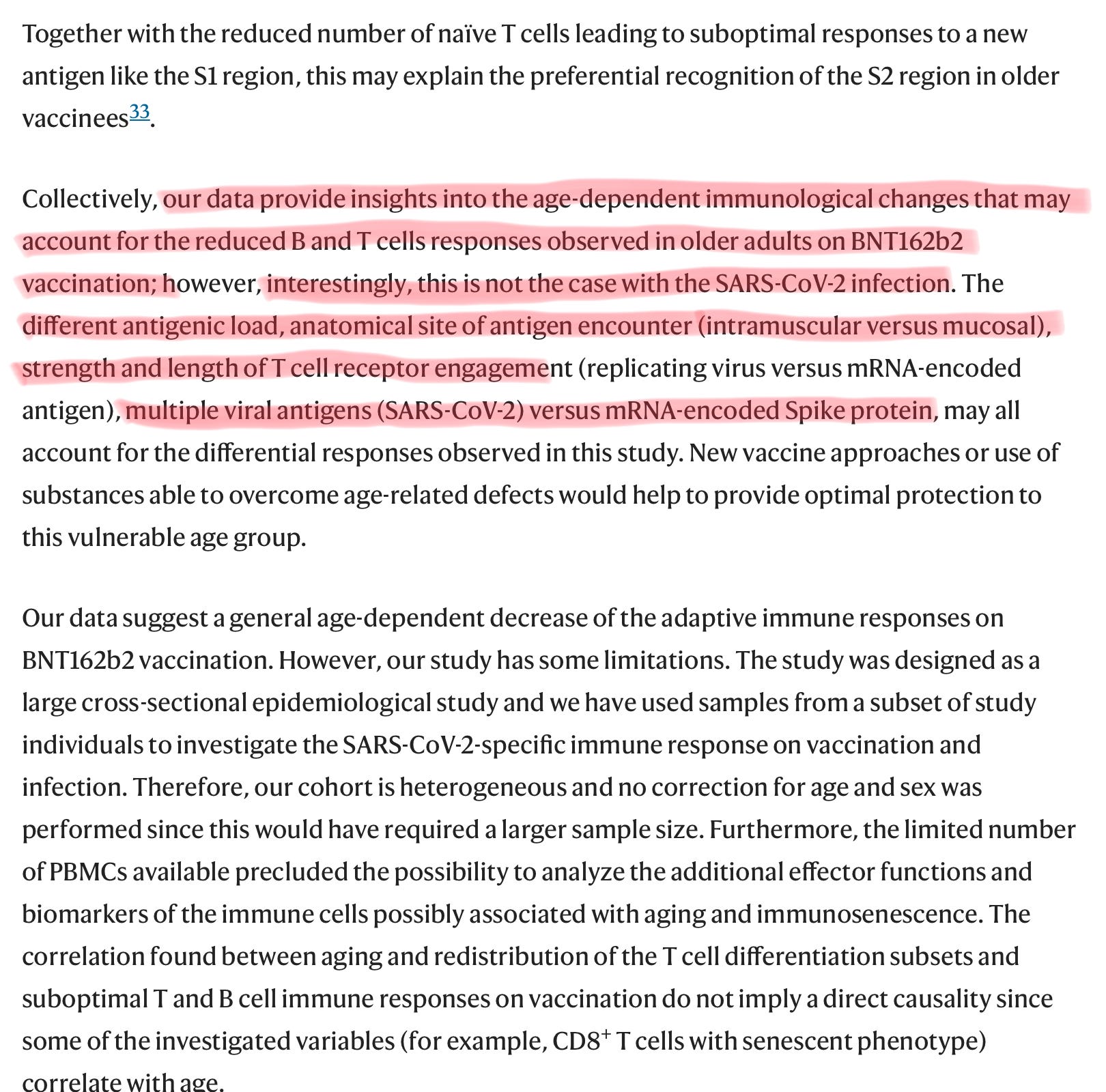
Here the authors argue a somewhat moot point now, the differences between natural infection and mRNA vaccination. But here is the reason I decided to write this one, not only both papers were published within almost 24 hours of each other, they fall into the subject I have been covering for a few weeks now, the shift in immune responses in regards to the mRNA vaccine, and its inflammatory properties. And the following, which if you didn’t read, I highly recommend you do it right now.
After reading it, what is more likely:
The mRNA vaccine is failing in older people because of their old age, and loss of “immune power”
The mRNA is failing because it chose a single protein (the Spike Protein) and the body is fixated on it, and since the immunity provided is not a sterilizing one, leads to further inflammation
The mRNA itself is setting off inflammaging, the breakthrough infections add to the fire, and since most older people have a decaying immune function, this leads to a form of chronic infection
So why did we vaccinated old people if it is borderline useless by now ?
And in case you are older, or wondering after reading this, and the Inflammaging one (super important), simple steps to tackle any possible problem arising from this.
A less inflammatory diet, like a low carbohydrate diet (older people thrive on it)
Intermittent fasting and fasting in general from 24 to 72 hours (start low)
GlyNAC is a must for older people as I recently covered, and for infected/vaccinated
Vitamin D+K2 after any form of viral infection
Proteolytic enzymes such as Nattokinase and Serrapeptase
Berberine helps among a dozen other things, with senescence too
I hope you have a good Sunday, maybe no post tomorrow, or something unrelated to biology/medicine.
Appreciate all supporters who enable me to do this and subscribers who share ! Thank you !
Although most of this goes over my head, I figured I’d say a big thank you for your comprehensive analysis on this. My takeaway is that I’m glad I avoided taking the jabs (despite the high personal cost as a citizen here in Chinada). Taking care of ourselves with diet, exercise etc also seems to be more important than ever. Thanks again for all your diligent work and for sharing with us. I’m sure it’s frustrating when you’re swimming against the current. Cheers!
Excellent thanks. The elderly who need it most get the least benefit. The catch 22 of immunology being that immunosenescence stops it working effectively, apart from creating systemic inflammation, TH17, K-RAS activation & tumorigenesis as just as a small part of the picture.