
More antigenic sin, immune shift in persistent infection
And Paxlovid is useless !

In case you don’t follow me on Twitter, I got a respiratory infection, and given the incidence of SARS-CoV-2 in my area right now, it was probably a new variant or something. Wrecked me in different ways, drained me of energy, and for the first time I can remember 3-4 days straight of fever, with the last 40 hours sweating (which is a good sign for me, clearing the infection in my case) and my brain literally couldn’t function for a couple of days in the weekend.
I now recovered enough cognitive function that I can think… somewhat. I do not see any reason to delve as deep as I usually do with these papers because I will just end up repeating myself. Yet again, we find ourselves with more evidence of things we already knew, with the first being more Antigenic sin evidence (per what I wrote earlier, that these papers would be published in batches within weeks).
In line with previously published evidence and using a couple of recent-ish variants to test antibody responses, their findings fall in line which what common sense told anyone instincts in 2020. Even breakthrough infections have a limited effect on how many effective antibodies the vaccinated body is able to produce, with not much improvement (meaning the vaccinated body is not picking up the new mutations, since it learned and is now fixated in one specific protein).
I like the term they used “ceiling effect” meaning the body has reached the pick of producing specific antibodies that are not that effective, this paper together with others (ones studying the shift in B-Cell responses) explain the shift in mRNA immunity, why there was a global immunological shift towards IgG 4, called “class switch”, an almost anti-inflammatory antibody.
Authors raise a point that researchers covering this, some molecular biologists months and everyone in between did, fixating on conserved epitopes is by now a fool’s errand, everyone’s immune system already learned what they needed from the virus, and the natural antibodies that cross-neutralized can’t be pumped out indefinitely, otherwise you get class switch.
The second paper I wanted to cover is the following. Oligosymptomatic means the person had few symptoms.
Oligosymptomatic long-term carriers of SARS-CoV-2 display impaired innate resistance and high Spike-specific neutralizing antibodies

Authors intended to elucidate why some people who have few symptoms became long-term carriers of the virus, shedding and infecting people longer than the normal average, without being immunocompromised. Here they identified that the initial immune response is somewhat impaired in these people.

Long-term carriers had a change in their monocytes populations, a drop in classical and a modest increase in non-classical monocytes (CD16 positive, meaning they have Fc gamma IIIa receptor), followed by finding a significant reduction in Plasmacytoid dendritic cells (pDC) a subset of Dendritic cells specialized in producing type I interferon. From all the cytokines measured (per the image above) the only one significantly different was IL-10, lower in the P (persistent-long term carrier) than the other two groups ( Non-Infected/NI, Non-persistent/NP), and unlike the other 2 groups, the Persistently infected group did not have an increase in tissue growth factors.
Means a weak antiviral response, and limited tissue repair in the first few days of the infection prolonged SARS-CoV-2 presence in the body. This is where it gets… interesting.
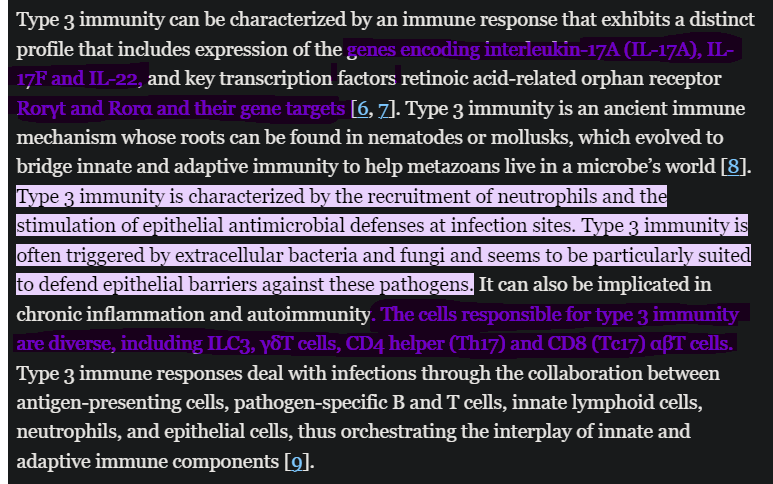
Type 1 responses shift to type 3 immunity in long-term carriers
Further analysis of systemic hallmarks of type 1 immunity revealed significantly lower IFNγ and IL-12 concentrations in the plasma of long-term carriers, but higher circulating levels of IL-15, a broadly pleiotropic cytokine with stimulating effects on NK cells and T lymphocytes. Considering the reduced type 1 immunity taking place only in the of patients subsequently evolving towards a persistent infection, we next explored whether long-term carriers presented a functional deviation to type 2 or type 3 immunity. Analysis of plasma cytokines showed that, while type 2-associated cytokines, such as IL-4, IL-13 and IL-9, were poorly represented in the plasma of patients with prolonged infection, the concentration of IL-17A was strongly increased . Soluble mediators responsible for neutrophil development and recruitment, such as G-CSF, MIP-1α (CCL4) and IL-8 (CXCL8) were also augmented, indicating a more prominent type 3 immune profile. These observations suggest a shift from type 1 immunity to type 3 immune 231 responses in patients with persistent SARS-CoV-2 infection.
Patients with Persistent infection not only had a weaker first immune response but shifted towards Type 3 immunity. From here.
Finally, fold change importance analysis performed on NP versus P patients highlighted IL-17A, MIP1α, IL-15, IL-8 and IFNγ as the top five cytokines defining SARS-CoV-2 persistency
Given what we know so far about the Spike Protein interacting with LPS and bursting biofilms via S1 interaction, one would have to wonder if the shift in the immune response to Type 3 is not merely against the virus, but also against bacteria and LPS that decorates the Spike like a Christima’s tree.
Also worth noting is the exact cytokine profile when compared NP versus P, almost exactly the same response the vaccinated have, which begs the question. Could this explain the partial debacle of getting the vaccine>soon after getting infected>spreading the virus more than non-vaccinated counterparts ?
In the discussion section of the paper, the author state that long-term (persistent) carrier displayed a shifted immune state, with increased IL-17A, 8, and other neutrophil-related chemokines, and I quote “In line with our data, mouse models of chronic infection by TMEV also link Th17 cells to viral persistence”. This is fantastic, the exact immune response a sizable portion of the vaccinated, and broken through experience, is the one that leads to viral persistence, besides all the other horrendous effects higher levels of Th17 for too long entails.
(For the record, these cytokines are pretty much the same and more abundant when LPS is present in your body).
I could finish this in many ways, but I will let the authors speak for themselves.
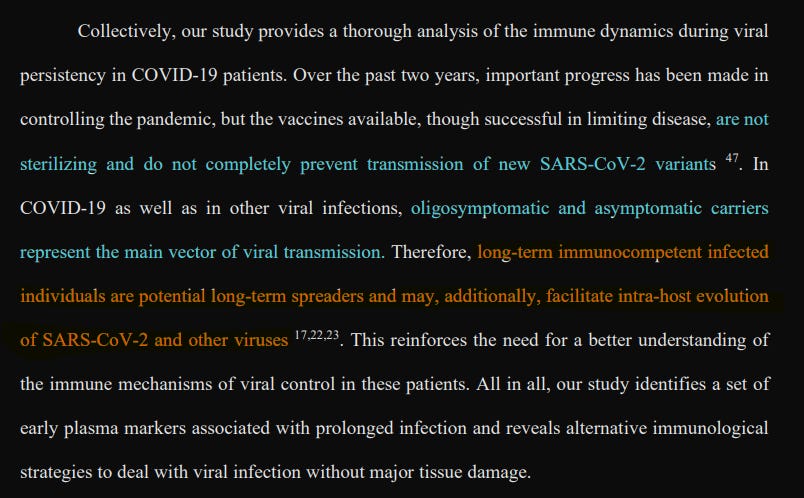
Fantastic huh. I would love to know the kynurenine/tryptophan and KP metabolites differences between the non-persistent and persistent groups too, among other markers.
And the last one for my own sake, and laughs, because I do love to be proved right, AND dunk on Pfizer moronic “scientists”.
Paxlovid-like nirmatrelvir/ritonavir fails to block SARS-CoV-2 transmission in ferrets
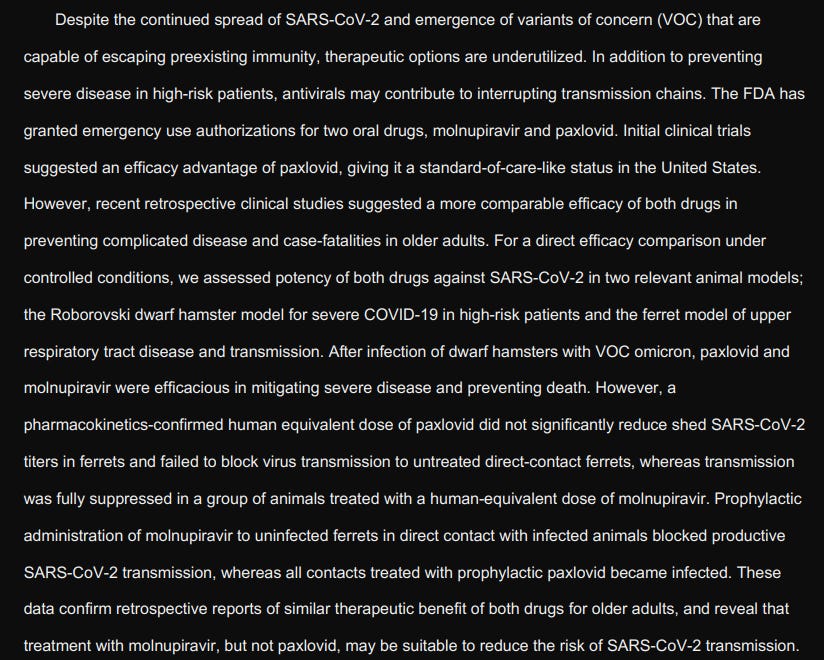
As I said months ago, Paxlovid is useless at best, dangerous-mutation fueling at worse. Pfizer’s business model is remarkable and does induce some level of envy in me because none of their proposed treatments actually works, and they keep making billions upon billions every quarter.
As a closing note to this substack, I will leave my opinion that I abhor what will happen with the new vaccines, they might not use the entire Spike Protein, but the parts they chose to develop are as bad because they are, partially, what signals the exact pathways that induce damage and disease.
Gotta gather all the data they need for as long as they can I guess.
I welcome and appreciate the support of those who choose a paid subscription, or who decide to buy me a coffee whenever they feel like it, and everyone who shares my Substack. Without all of you, this wouldn’t be possible.
I’m glad you’re feeling better. Prayers for your full recovery.
My brother’s 62 year old patient who had taken 2 original shots of mRNA recently died of covid. She was on day 3 of Paxlovid when she died. My brother, who is an obedient follower of CDC, said she wouldn’t have died if she had taken the bivalent booster. He is shocked she died, but refuses to be open to reading about early treatment protocols I’ve tried to point him to.
I haven’t finished this post. Just wanted to say that I am dreadfully sorry you have been sick. I am very concerned for the rest of us as well. Be well