


IgG4, Long Covid, and the road to Rome
All roads end there...

A good choice of songs to read this piece.
This is directly correlated with the following piece, it also plays a role on the ADE scenario, and will also play a major role in the Protein Mimicry one. Understanding the shift towards IgG4 and what it entails is paramount to understanding 2023 and onwards, even if vaccination rates go to 0.

Published just a couple of days ago, the following paper instantly caught my attention.
The patient described here “71-year-old male with hypertension, coronary artery disease, prostate cancer and chronic obstructive pulmonary disease with a 50-pack year smoking history”, the smoking ends up being almost a pack a day.
7 days after receiving the Pfizer mRNA vaccine with some pulmonary problem. 2 weeks after the second dose, he went to the emergency room and after tests attending doctors saw hypoxia and put him on 3L of oxygen. Meaning he lost pulmonary function. Loss of function persisted after 3 months of treatment, ending up with the patient using 5L of oxygen.
Up until today, there are very few reported and published cases of IgG4-related diseases in relation to the mRNA vaccination, but as the authors, themselves bring to our attention diseases linked to IgG4 are underdiagnosed and actually hard to diagnose most of the time, I think an honest deduction is there are at least dozens, if not a few hundred cases already. The IgG4-related nephritis relapse can be found here.
One of the most widely accepted aspects of the mRNA vaccines is the “heart disease” angle, it is almost impossible to deny, no matter how much the media pushes for it, so I decided to go a little further.
IgG4 related cardiac disease
Pseudotumors involving the heart have been reported but have not been shown to be related to IgG4 disease. Although there was no pathology confirmation of heart involvement, the nature and extent of the organ involvement led us to conclude that it was due to IgG4-related disease. The use of the PET scan may help identify involvement of the myocardium.
Immunoglobulin G4-Related Cardiovascular Diseases
Immunoglobulin (Ig) G4-related diseases are a new concept and affect a variety of different organs. Organs that may be affected include the pancreas, bile duct, lacrimal glands, salivary glands, central nervous system, thyroid, lung, liver, gastrointestinal tract, kidney, prostate, retroperitoneum, cardiovascular system, lymph nodes, skin, and breast. IgG4-related disease presents with a variety of symptoms according to the organ affected, and may be accompanied by serious complications such as organ dysfunction associated with IgG4 positive cell proliferation. IgG4-related cardiovascular diseases affect the coronary arteries, heart valves, myocardium, pericardium, aorta, and peripheral vasculature. Herein, we review IgG4-related cardiovascular diseases.
Does the list of damage in the heart in relation to IgG4 remind you of anything else ? Plus the list of organs affected by IgG4 is quite remarkable isn’t it.
Since there is an undeniable correlation between a lot of the conditions and diseases IgG4 can fuel and lead to progression, I decided to let my gut and my bias take the better of me and see if there was any correlation between immune cells activating or inducing IgG4. Well, to my sincere surprise, our oldest friend was there once again. IL-17. Th17. To be relatively sure about it.
Roles of IL-17, Th1, and Tc1 cells in patients with IgG4-related sclerosing sialadenitis
Conclusions: Increases in Th1 and Tc1 cell populations and IL-17 expression might be involved in the mechanism of pathogenesis of IgG4-related sclerosing sialadenitis.
Now, to further bring my point to your attention, there has been quite a discussion among some clinicians and researchers about IgG4 and SARS-CoV-2 infection.
From here.
In this prospective study we found that serum IgG4 level predicts a poor COVID-19 outcome. Based on the available literature, IgG4 antibodies may contribute to COVID-19 progression via at least two possible mechanisms, yet to be verified. Because anti-spike IgG4 have shown poor in vitro neutralizing capacity compared to IgG1, IgG2, and IgG3 antibodies, a first possibility is that hosts with prominent IgG4 immune responses might be more permissive to SARS-CoV-2 infection [6]. On the other hand, as neutralizing anti-IFNγ autoantibodies observed in adult patients with multiple opportunistic infections are predominantly of IgG4 subclass, it is tempting to speculate that anti-IFN antibodies associated with impaired anti-SARS-CoV-2 immunity and life-threatening COVID-19 pneumonia might also be IgG4 [7]. Despite intrinsic limitations mainly related to the limited number of patients enrolled, our study identifies IgG4 antibodies as a possible additional overlooked variable of the humoral immune response against SARS-CoV-2 associated with COVID-19 progression.
And here.
Indeed, IgG4 elevation in the context of high IL-6 levels has been already reported in other inflammatory disorders such as Castelman's disease, suggesting that the increase of serum IgG4 observed in hyper-inflamed COVID-19 patients more likely represents an intrinsic disease feature rather than an occasional finding related to other causes
May IgG4-related disease be reactivated by SARS-CoV-2 infection?
Herein, we report disease activation in an IgG4-related patient in remission as a result of SARS-CoV-2 infection
It has been recently corroborated by multi-centre study in Europe that patients IgG4 related diseases will have a poorer outcome with the disease.
My argument here is not IgG4 being the sole driver of severity and mortality, but as I have been writing for months, disease acceleration and creation, as a friend named it “The Great Accelerator”. In this context, the evidence is numerous, extensive, and quite clear in the presence of high levels of IgG4 and poor neutralization, adding a pinch of molecular mimicry, it will definitely feed disease and it is related under certain circumstances to Interleukin-17 (therefore Th17). A recent paper argued a similar mechanism, using different molecular pathways, but it is directly correlated with the “BA. 5 Spike is a bad vaccine target” piece.
Now you may be asking yourself what this has to do with Long-Covid, besides me pointing out many times that vaccination is one of the causes of Long Covid (since the main drivers of the inflammatory state that induces LC is the same in the viral infection, the S Protein).
And before I mention the following paper, I don’t think Long-Covid has a unique cause, it is a complex multi-factorial disease, but there are clear inflammatory trends among a lot of people with LC, and a lot of them get remarkably better after 4 to 8 weeks of addressing these causes.
The entire paper is worth reading because it gives you a lot of insights into how unique PASC (Long Covid) can be, and gives more credence to the argument that this is not merely a dysregulation of the immune system, but also disease acceleration.
Liquid biomarkers of macrophage dysregulation and circulating spike protein illustrate the biological heterogeneity in patients with post-acute sequelae of COVID-19
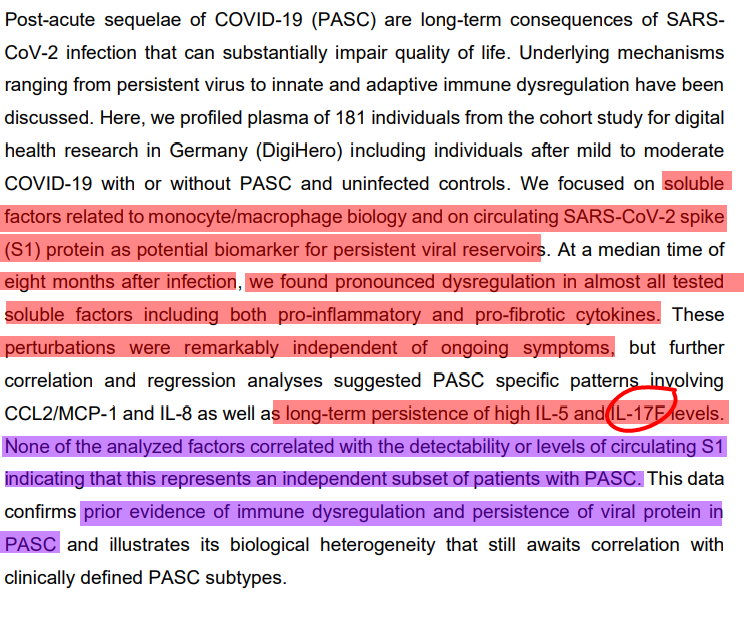

In a portion of the patients, they didn’t find a strong correlation between S1 floating around and the immune state the patient found themselves in, therefore creating a new subset of Long Haulers. But the most remarkable finding was the persistently high levels of IL-17, among other markers even 8 months after the onset of symptoms.
Now here is the “kicker”, and to not overcomplicate a topic that is already incredibly complex given how I have been putting this together. IL-33, and IL-18 will both cause differentiation of cells towards Th17 under certain circumstances but one of the biggest known drivers of Th17 besides its sister cytokine (IL-17) is IL-23.
These cytokines create two subsets of Long Haulers in the same paper, one is more prone towards a more “allergic” response, which many people who talk to me in my DMs find themselves, and the other is the low-grade long-term inflammatory, profibrotic state.
This is one of the reasons just a few supplements can cause big improvements in so many people (VitaminD+K2, Berberine/Metformin, Glycine+NAC, which I will write an entire piece solely on this one, and enzymes such as Serrapeptase/Nattokinase). The best way to address or avoid this IgG4 disease acceleration process is to address the causes of it, and the immune dysfunction, especially if the person is vaccinated multiple times. After each infection, high doses of antioxidants, and higher doses of the other supplements to avoid the progression of any underlying, subclinical damage.
I will leave this here as a “forecast”, within months not only the number of IgG4-related diseases will “suddenly, inexplicably increase” but they will find a strong correlation in many of the 4 times plus vaccinated and Long Covid, and after that IgG4 and Long Covid in a sizable portion of people.
As I have been hitting for days now, I will take as long as I need meaning probably until Friday or Saturday to write my Protein Mimicry piece, because it will tie all of this together. At the end of that piece, you will understand how this IgG4 shift truly is.
As the last addition, from the following piece. All roads lead to Rome (Th17), and Rome has a bioenergetic problem.
In the end, as much as I wish I could find one, singular pathway to solve the entire etiology of this disease, I will never be able too, and nobody intellectually honest will say they will. The spike protein itself has so many things from different sources and so many protein (mimicry) like ours, it’s a Clausewitzian molecular war.
I still hold the opinion that this is one of the most significant aspects of this disease (and many others, in fact, mitochondrial dysfunction causes and worsens the progression of many many diseases). In my opinion, the massive replication of all current variants, the massive amount of ROS generated, persistent low-grade inflammation, and immune dysfunction contribute to this.
This dysfunction itself leads to senescence, one thing feeds the other. While not the end all, be all, for me, it’s one of the most important aspects, and why supplements that aid mitochondrial function brings relief to many people post-Covid (whatever degree of severity they find themselves in).
Big thank you as usual for all my supporters, you are all amazing people ! And the ones who often share my posts too !
Increased IgG4 means suppressed Immune response to spike protein from covid or vaxx and general autoimmunity wherever the mRNA goes in the body. This has to be the worst product ever brought to market.
Oh my, have you seen this review Brian Mowrey took on at my request, or the underlying paper concerning IgG4 out of Germany which is linked to in the review? More pieces falling into place here.... bottom line is that our immune systems start to tap out from creating functioning, "inflammatory" IgG1-3 type antibodies in a big way after 3rd booster.
https://unglossed.substack.com/p/boosting-tolerance-igg4
edit: sorry.. I now see that you did address the German paper in your Sept. 10 post... anyway, Brian's piece remains as companion commentary.