
Creatine supplementation improving Long Covid symptoms
And a lot more

I have been waiting for a while to write a bigger article on this subject, I wasn’t exactly holding back, but waiting for some level of good evidence, and this also adds to one observation I mentioned multiple times, to multiple people. Sometimes supplements take time to “work”, and from experience, more often than not it takes months, which is a problem since people start chasing rabbit roles of their own making and jumping from “protocol to protocol” every other month.
Effects of six-month creatine supplementation on patient- and clinician-reported outcomes, and tissue creatine levels in patients with post-COVID-19 fatigue syndrome
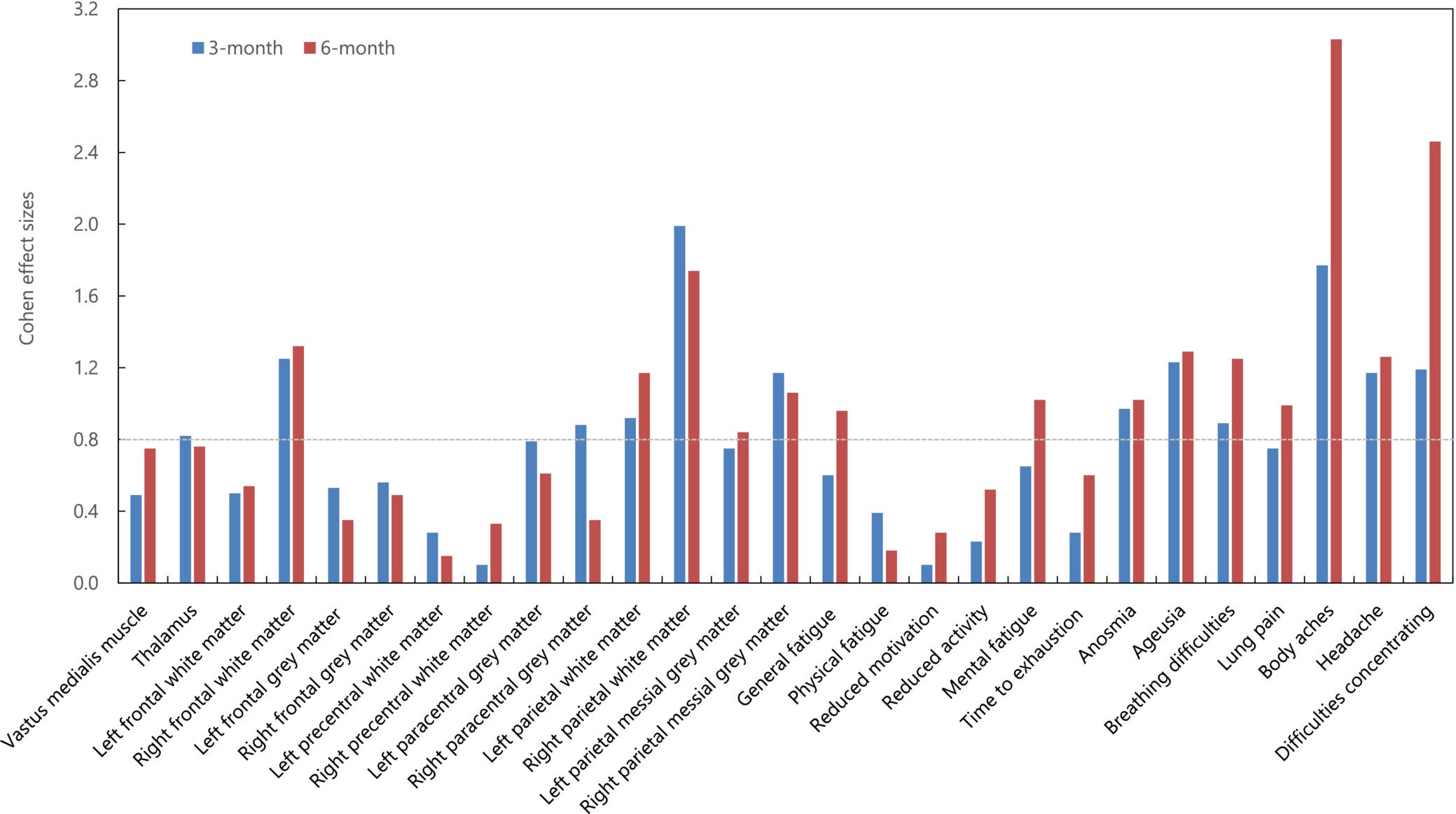
Dietary creatine has been recently put forward as a possible intervention strategy to reduce post-COVID-19 fatigue syndrome yet no clinical study so far evaluated its efficacy and safety for this perplexing condition. In this parallel-group, randomized placebo-controlled double-blind trial, we analyzed the effects of 6-month creatine supplementation (4 g of creatine monohydrate per day) on various patient- and clinician-reported outcomes, and tissue creatine levels in 12 patients with post-COVID-19 fatigue syndrome. Creatine intake induced a significant increase in tissue creatine levels in vastus medialis muscle and right parietal white matter compared to the baseline values at both 3-month and 6-month follow-ups (p < .05). Two-way analysis of variance with repeated measures revealed a significant difference (treatment vs. time interaction) between interventions in tissue creatine levels (p < .05), with the creatine group was superior to placebo to augment creatine levels at vastus medialis muscle, left frontal white matter, and right parietal white matter. Creatine supplementation induced a significant reduction in general fatigue after 3 months of intake compared to baseline values (p = .04), and significantly improved scores for several post-COVID-19 fatigue syndrome-related symptoms (e.g., ageusia, breathing difficulties, body aches, headache, and difficulties concentrating) at 6-month follow-up (p < .05). Taking creatine for 6 months appears to improve tissue bioenergetics and attenuate clinical features of post-COVID-19 fatigue syndrome; additional studies are warranted to confirm our findings in various post-COVID-19 cohorts.
While done with a small group (12 patients) it falls in line with personal, group, clinical, and scientific observation. Besides the statistical talk, the paper is pretty straightforward to understand, Creatine supplementation for a long period significantly improves a few of the worst symptoms of Long Covid, especially at 6 months when the authors observed improved tissue bioenergetics.
Put simply, the muscles achieve proper “energy generation and use”, the opposite (fatigue, especially severe fatigue, muscle pain, “brain fog”) being a hallmark of poor bioenergetics. To my surprise, the dosage used is vastly below what I would expect for such remarkable improvement. 4 grams per day, 5 grams per day is the “average” dosage for most people who make use of creatine. This dosage is also cost-effective since the body has a (biokinetic) cap on amino-acid absorption, especially in supplement form, it is fairly unique to eating a lot of meat, where animal protein digestion is slow and the amount of amino acids absorbed by the body is vastly different than taking as a supplement (aka therapeutic dosage). As a simple rule of thumb, 10 grams of amino acids per 4 hours is the human body cap when taken power+liquids (diluted in said liquid).
Before delving any further, the best method to take creatine is with a carbohydrate source, since insulin helps with the transport of the amino acid into blood circulation and muscles. Timing doesn’t matter much, some prefer in the morning, others late at night. I personally prefer it in the mornings.
The Discussion section of this paper refers to other trials done by other groups with different dosages, but similar improvements.
CONCLUSION
Taking creatine for 6 months appears to improve tissue bioenergetics and attenuate clinical features of post-COVID-19 fatigue syndrome, possibly due to its energy-replenishing and neuroprotective activity. Endorsing creatine might be thus of great importance in tackling highly prevalent PVFS after COVID-19 pandemics; additional studies are warranted to confirm our findings in various post-COVID-19 cohorts.
Now we do what we usually do. A deluge of useful information. If there is one supplement I advise any human being to take, long-term, is creatine.
In the article “How to deal with Latent infections” I wrote the following and dozens of mentions of creatine to treat many conditions in my now defunct Twitter profile.
While I still need to dedicate an entire piece to certain amino acids, creatine has been proposed for decades to prevent herpes recurrences, creatine has many uses but one of the most pertinent effects is its effects on CD8 (basically the cells that keep latent viruses, well, latent, in a simplistic manner), these cells also are the first to go into a dysfunctional state during reactivation.
As in the quotation above from another article, one of the most interesting aspects of creatine is the effect on killer cells, creatine uptake (a cell “grabbing” creatine to use it) is necessary for CD8 cells to kill cancer cells, as a byproduct, it is also useful to keep latent viruses in latency. Creatine supplementation effectively suppressed tumor growth by drastically reducing the number of PD-1hiCD62Llo cells (an “exhaustion-prone” T cell phenotype) among the tumor-infiltrating CD8 T cells. Two birds, one amino acid stone.
Creatine Alleviates Doxorubicin-Induced Liver Damage by Inhibiting Liver Fibrosis, Inflammation, Oxidative Stress, and Cellular Senescence. Creatine also possesses anti-depression effects. In another study, the authors found the following positive effects on microvasculature.
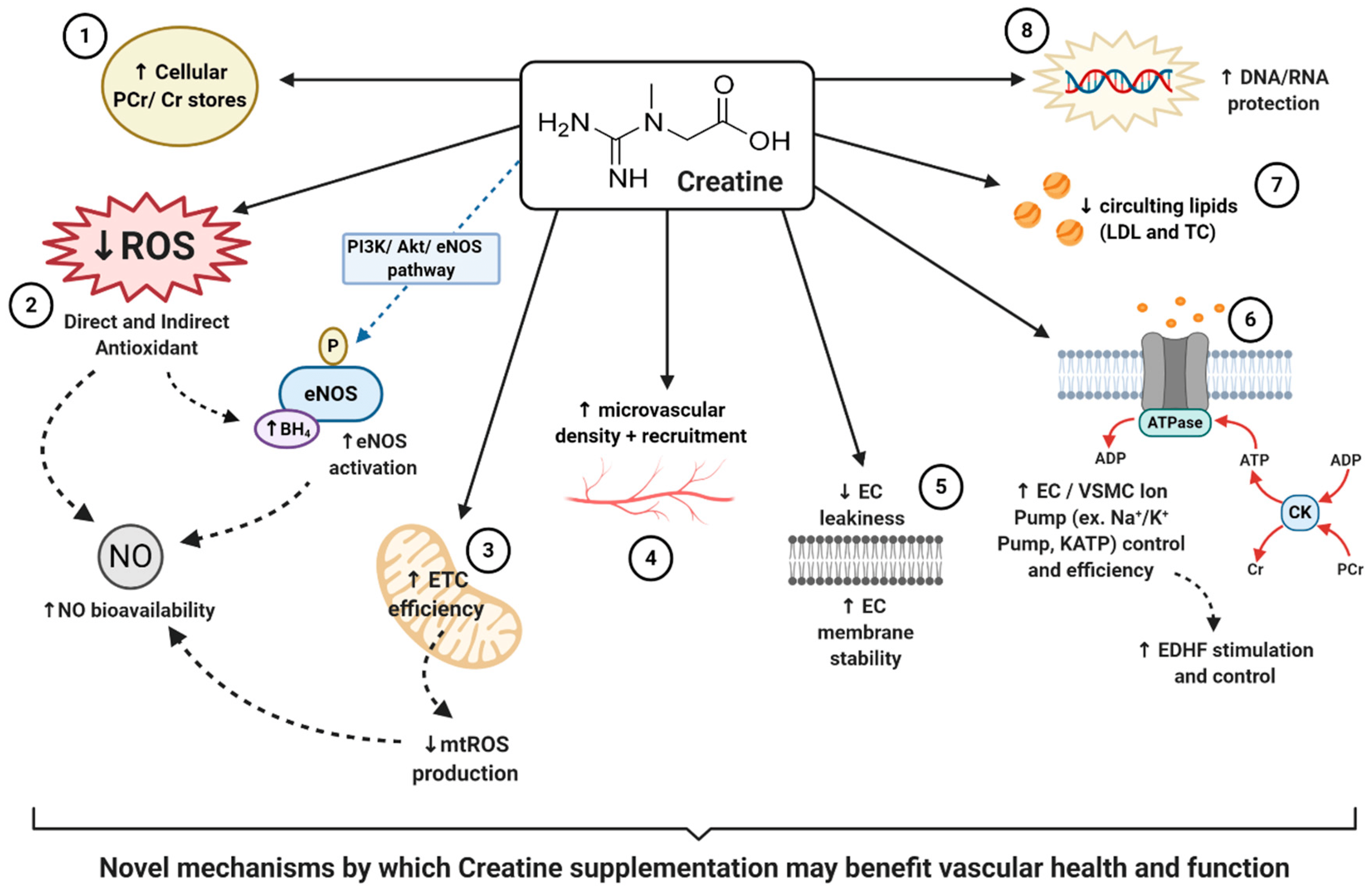
The main findings of this study are as follows: i) oral supplementation with creatine monohydrate in healthy, moderately physically active young adults improves systemic endothelial-dependent microvascular reactivity; ii) the supplementation also increased skin capillary density and recruitment, which are dependent on microvascular endothelial function; and iii) blood pressure was also reduced after the supplementation.
Therefore creatine has both direct and indirect effects, and partially some of its positive vascular effects come from affecting Nitric Oxide and its synthesis. Further information on the impact of creatine in older adult’s endothelial function, “Our findings indicate that 4 weeks of creatine supplementation, but not placebo, improves endothelial function and microvascular reactivity in older adults; however, there was no benefit for arterial stiffness. Creatine supplementation, in comparison to placebo, can also improve markers of short-term memory and isokinetic muscle endurance, but neither creatine or placebo improved visuospatial awareness or isokinetic muscle strength.”
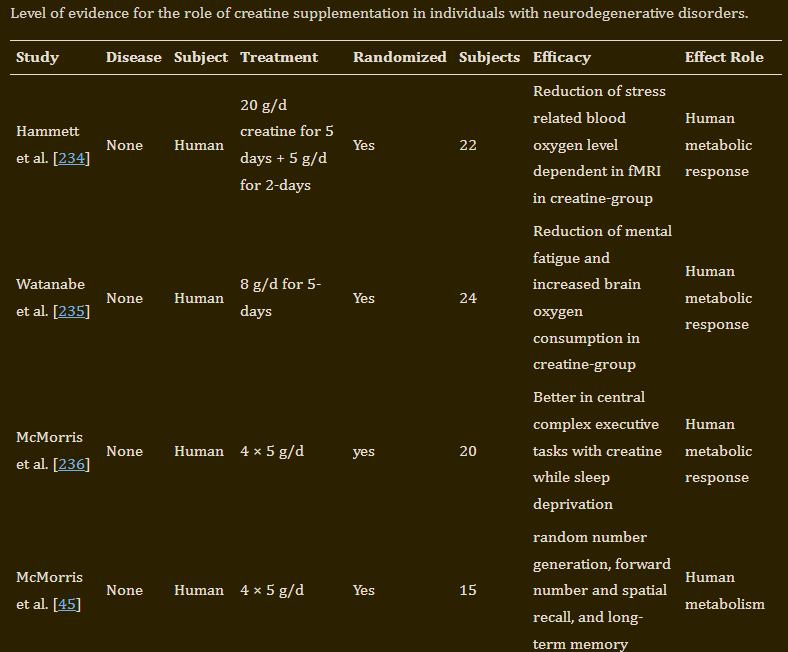
Creatine supplementation also has significant effects on brain function and health (cited papers on positive effects from the paper linked 23,62,63,64,65,66,67,68,69,70,71,72), an extensive review can be found here, covering the effects of the supplement in Traumatic Brain Injury, Alzheimer’s, Parkinson’s, Multiple Sclerosis, Amyotrophic Lateral Sclerosis, other muscular dystrophies and mood disorders. While the cause of each condition is both complex and fairly “unique”, their progression and the worsening of each person afflicted by these conditions stems from similar pathways.
A substantial oxidative burden directly impacts energy generation on both cells and tissue (muscle or otherwise), therefore throwing the entire physiology into a cascading bioenergetic loss, leading to loss of immune tolerance, excessive cell death of the wrong cells, and more inflammation. Creatine acts directly into ATP (energy generation) being one of the best long-term supports for proper bioenergetic function, so creatine is able to offset the energy loss and support systemic function, especially muscular function.
While I usually recommend reading all cited papers for a comprehensive understanding of all the matters discussed in this Substack, I understand often it is often outside the reach of many people, yet in this particular case, I highly recommend, even if you don’t fully understand, to read the following paper. Why ? Because of the matters discussed, mitochondrial dysfunction and its dynamics are at the core of many, if not most modern diseases. Mitochondrial function goes beyond “necessary”, it is primordial to life.
Role of Creatine Supplementation in Conditions Involving Mitochondrial Dysfunction: A Narrative Review
Numerous studies over the last three decades have shown that creatine monohydrate (CrM) supplementation (e.g., 4 × 5 g/day for 5–7 days or 3–6 g/day for 4–12 weeks) increases muscle creatine and PCr content by 20–40% [5,11,12,13,14,15] and brain creatine content by 5–15% [16,17,18,19,20,21]. Creatine monohydrate supplementation has been reported to safely improve high-intensity exercise performance by 10–20% leading to greater training adaptations in adolescents [22,23,24,25,26], young adults [27,28,29,30,31,32,33,34,35,36,37,38], and older individuals [21,39,40,41,42,43,44,45,46,47,48]. No clinically significant side effects have been reported other than a desired weight gain [49].
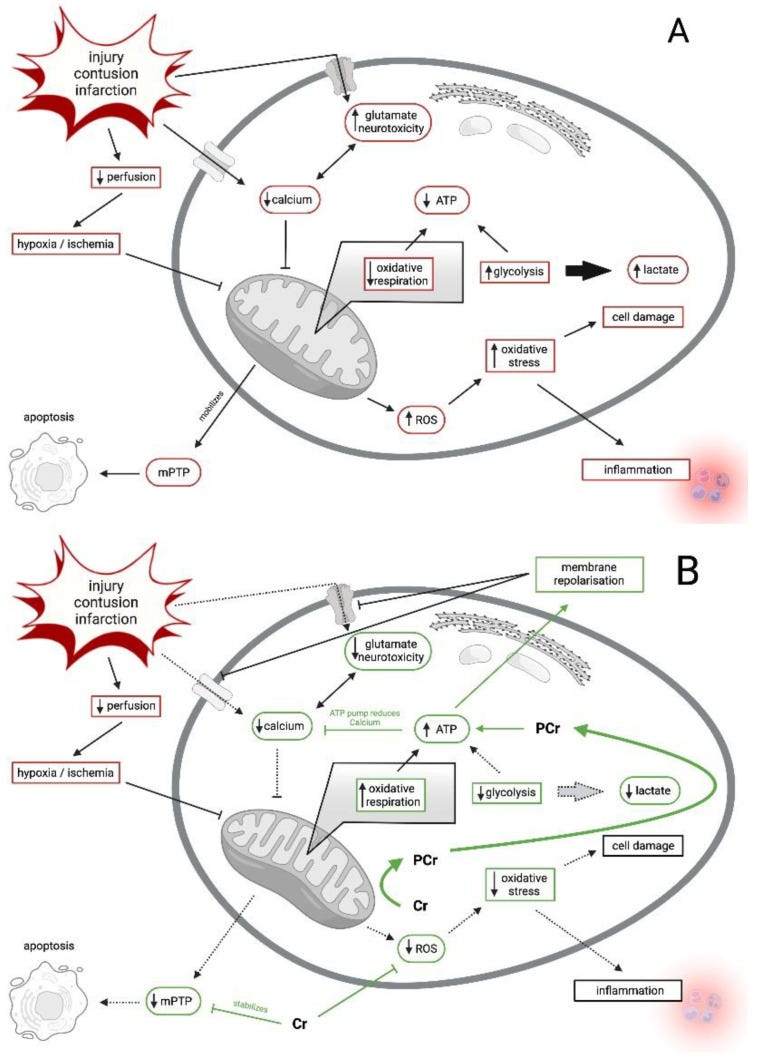


The most important section of this paper from my perspective is the 3.2 Chronic, Atraumatic Mitochondrial Dysfunction. The authors describe pretty well how chronic mitochondrial dysfunction often happens, usually be slow, progressive changes in mitochondrial dynamics, eventually leading to increased ROS, glycolysis, and more glycolysis leads to acidosis, these changes affect both mitochondrial shape (incredibly important) and mitochondrial function, the capacity to properly and efficiently generate energy. Hypoxia also plays a significant role in mitochondrial decay (dysfunction), many conditions affect hypoxia, such as clots, tumors, and inflammation.
The ultimate, most common denominators are reactive species which damage mtDNA. As soon as cellular defense systems such as antioxidants, intracellular energetic buffer, and enzymatic reactions are worn down, chronic alteration of cellular organelles begins [116]. As mentioned above, it is hard to differentiate in chronic mitochondrial dysfunction whether pathological conditions lead to hypoxia that produces ROS/NOS which eventually harms mtDNA or whether an altered mtDNA leads to an overexpression of ROS/NOS damaging itself [117]. It is widely accepted, however, that this chronic status is a vicious circle leading to a lethal cellular condition harming the host.
The following section is the most impactful and significant to this conversation, and arguably to 70% of the pathways I covered.
Creatine is able to buffer lactate accumulation by reducing the need for glycolysis [126], reducing ROS [127] and restoring calcium homeostasis.
Creatine can “reverse” the Warburg Effect to a level, helping restore efficient energy production, and proper calcium flow (as I wrote multiple times in my mitochondria-centered articles, proper intracellular calcium is arguably one of the most important aspects of mitochondrial health), and by helping rescue proper bioenergetics it lowers ROS, and lactate (a marker of many inflammatory and diseases). Among the dozens of physiological effects Endotoxins (LPS) and sepsis cause, one of the most important is a shift toward the Warburg Effect, and the other is the dysregulation of neutrophils.
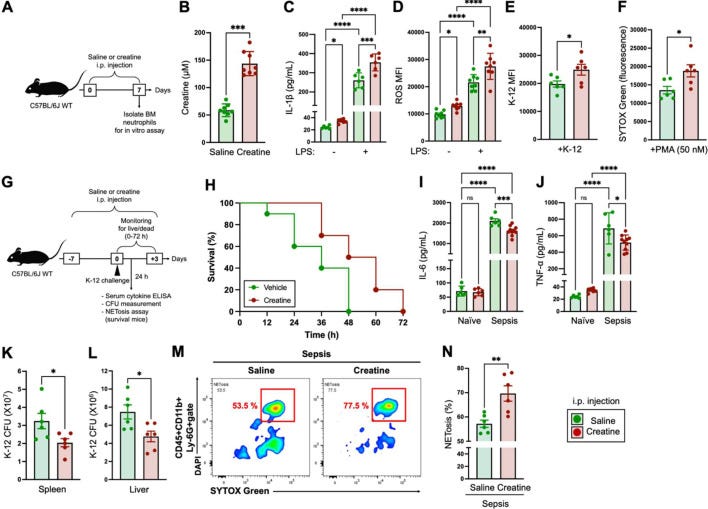
Creatine supplementation enhances immunological function of neutrophils by increasing cellular adenosine triphosphate
Creatine is an organic compound which is utilized in biological activities, especially for adenosine triphosphate (ATP) production in the phosphocreatine system. This is a well-known biochemical reaction that is generally recognized as being mainly driven in specific parts of the body, such as the skeletal muscle and brain. However, our report shows a novel aspect of creatine utilization and ATP synthesis in innate immune cells. Creatine supplementation enhanced immune responses in neutrophils, such as cytokine production, reactive oxygen species (ROS) production, phagocytosis, and NETosis, which were characterized as antibacterial activities. This creatine-induced functional upregulation of neutrophils provided a protective effect in a murine bacterial sepsis model. The mortality rate in mice challenged with Escherichia coli K-12 was decreased by creatine supplementation compared with the control treatment. Corresponding to this decrease in mortality, we found that creatine supplementation decreased blood pro-inflammatory cytokine levels and bacterial colonization in organs. Creatine supplementation significantly increased the cellular ATP level in neutrophils compared with the control treatment. This ATP increase was due to the phosphocreatine system in the creatine-treated neutrophils. In addition, extracellular creatine was used in this ATP synthesis, as inhibition of creatine uptake abolished the increase in ATP in the creatine-treated neutrophils. Thus, creatine is an effective nutrient for modifying the immunological function of neutrophils, which contributes to enhancement of antibacterial immunity.
As a byproduct of helping your cells properly function and produce energy in a more efficient manner, the positive effects cascade into a myriad of other “healing effects”, many of the conditions and dysfunctions linked to Long Covid are directly or indirectly targeted by creatine supplementation, ameliorating the symptoms and helping recovery.
Also, I often refrain from stating the obvious, but this time I will not.
One of the most obvious uses for creatine supplementation, for decades, has been aiding in exercise, especially recovery. It goes without saying given the subject covered in my last article that exercise+creatine, long-term are massive, powerful recovery tools, for many conditions, not merely Long Covid. Hopefully, together with the Exercise article, this proves to be helpful to some of my readers or their friends and aid their recovery, or just general health optimization.

After almost two years I discovered you can set different messages to each type of subscriber, but I still sometimes still say thanks for the support of paid subscribers. Thank you.
This is a fairly complex, but highly interesting paper -> Evidence suggesting creatine as a new central neurotransmitter: presence in synaptic vesicles, release upon stimulation, effects on cortical neurons and uptake into synaptosomes and synaptic vesicles
Per the title it proposes that creatine may be a new neurotransmitter
https://www.biorxiv.org/content/10.1101/2022.12.22.521565v4
JP, a number of years ago I found I had a Homocysteine level around 15. An MTHFR SNP or two. I reduced that Hcy level bit by bit with several items, each dropping the Hcy by about an average of 1.5 units. One was L-5-MTHF. Another was exercise. Creatine HCl was another. I found I could get enough Creatine with only about 1/8 tsp of the HCl form and believe that the creatine is packaged more efficiently in the HCl form than in the monohydrate form.
Do you know anything about the HCl form of creatine and how it compares to the monohydrate form? Are they just different forms of the same thing with similar or identical effects, or does each form have its own collection of effects? With the monohydrate form, one has to take many grams a day, which has been pretty expensive. I think I can get the same amount of creatine with significantly fewer grams of the HCl form but have never really understood the difference between the two forms or if there are differences in the amount of grams needed for energy and recovery effects versus how much I need to handle an Hcy overage problem.
Any thoughts on this? (Thanks!)