

I didn’t expect to write something so shortly, but since it fits pretty well the underlying themes of the last few articles, and the next few ones, and it is important information, here we are. This article will be much shorter and more direct, easier to understand than my usual. For a lot more information and a deeper discussion:

From personal experience to societal observation, one of my primary focus has been the brain. We now understand that the brain is not in an exclusion zone, safe from whatever otherwise occurs in the body. Protected, yes, safer, somewhat, impervious, absolutely not. Changes in the periphery (outside the nervous system) affect the brain, and vice versa.
From superficial memory, I have over a dozen articles with complex analyses of the effects of SARS-CoV-2, that can tangentially be expanded to the mRNA vaccine impact on the brain. My goal here is not to feed the doom and gloom hamster wheel of attention that moves society now but to bring awareness.
Post-COVID cognitive deficits at one year are global and associated with elevated brain injury markers and grey matter volume reduction: national prospective study
In an atypical outlying event, we are entering our fourth year in a pandemic. The average is 2 years, with the common exception of the Black Death (Bubonic Plague) which occurred on average every 400 years give or take, and lasted longer. Although short lived most pertinent lingering issue of the Spanish Flu was its contribution to neurological diseases.
This study had 351 Covid-CNS (neurological complications) and 2.927 in the “control group”. Average age 54, 89 had severe SARS-CoV-2, 57 were vaccinated against Covid before the infection. 190 of the 351, over half of the CNS group, had neurological or psychiatric complications associated with the infection. The NeuroCOVID group tended to experience milder symptoms than the “control” group and were assessed earlier in post-hospital admission.
Patients in all groups were significantly less accurate and slower in their responses, using a test to measure cognitive performance (Global Deviation from Expected-GDfE). As one would expect, the lowest scores were among the ones who suffered encephalopathy, and to a lesser extent cerebrovascular or inflammatory complications. Before the infection, 11 NeuroCOVID and 15 “normal COVID” patients were concerned about their memory, increasing to 84 for Neuro, and 66 for “normal”.

The pattern of cognitive impairment was generalized, meaning it didn’t matter much the group the patient belonged to, they all experienced impairment. Next, they measured recovery time, this was accompanied by other markers. In the NeuroCOVID group, a raised level of Tau (protein associated with cognitive decline and memory deficit) demonstrated reduced recovery.
Surprisingly to me and perhaps many others right now, in the “normal Covid” group, if infected by the earlier strains and had increased levels of UCH-L1, they also had lower recovery. This protein removes the “tagging” system the body uses to deal with unwanted proteins, therefore higher presence = more unwanted proteins around. Followed by imaging analysis, they found reduced grey matter volume in both groups.
I will leave the author’s own words as a closing remark.
our study found global, persistent cognitive deficits even in those without clinical neurological complications. When compared to normative age-matched data, these deficits were equivalent in magnitude to ageing from 50 to 70 years of age. This study indicated cognitive deficits were associated with the severity of the initial infective insult, post-acute mental health status, and a history of COVID-19 associated encephalopathy, with strong concordance between subjective and objective deficits. Despite some improvement at the first follow-up, by the second there was a plateau in the cognitive recovery trajectory and there was evidence of ongoing neuronal and astrocytic injury one year after acute COVID-19, even in those without neurological complications, with demonstration of underpinning neuroanatomical substrates.
The findings are both clinically significant and biologically plausible. Raised brain injury markers have been demonstrated in acute and post-acute COVID-19 and are associated with dysregulated innate and adaptive immune responses. The pattern of acute inflammatory proteins can predict post-acute cognitive outcomes and the finding, here, that acute treatment with corticosteroids may be protective for cognition is consistent with previous research, and further supports the hypothesis that brain injury in COVID-19 is immune-mediated. We have additionally shown that persistently raised serum GFAP was associated with post-acute cognitive impairment. GFAP is expressed by astrocytes, which participate in neuroimmune interactions within the brain. Its appearance in the plasma typically indicates injury of these cells and has been proposed as a prognostic biomarker for cognitive decline in the general population.
There is another study, fairly recent, that goes to great lengths to find the biological mechanisms for this persistent inflammatory response and dysfunction, I intend to cover it in the near future. As I and a friend often had long conversations about, SARS-CoV-2 is “The Great Accelerator”, and it will accelerate many diseases by the mere inflammatory response, let alone its synergy with many other pathogens.
Incidentally, the markers measured in this paper are also elevated, sometimes persistently for months after sepsis. It is called Sepsis-associated brain dysfunction (SABD). Here you can find a good review, that mentions one receptor specifically that I will come back to. RAGE.
I can not emphasize enough how proper antioxidation is paramount not just to your general health, but especially your brain health. Some of the markers discussed here have a close relationship with NRF2, the master regulator of antioxidantion, it will be central to the Glymphatic System Part II.
This obviously can be extrapolated to “how far ahead of the curve” a portion of the vaccinated are, but at this point, the evidence is mounting given the mix and match of immune responses and how absurdly fast the virus evolved, it will tax many. It will take many years, if not a couple of decades to fully comprehend that even the “mild” strains still induce damage, even if you get “just the sniffles”.
The particular reason I am sharing this research is not merely because of brain “stuff”, but because of the following. One of the biggest and longest-running arguments has been “Omicron is mild bro, it doesn’t get into the lungs bro, it doesn’t bind well to ACE2 anymore bro”.
Viral evolution aided by human stupidity is a heartless harlot. You can read a very recent “current vaccines are useless” (what I refer to as vaccine dunking) paper here. Findings are similar to the research below, newer strains can enter the lungs.

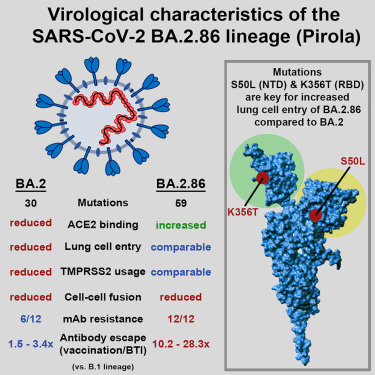
I know the vast majority will focus on the phrases with the word “vaccinated” here, especially with the booster-pushing syntax, but the fourth Highlight is where you should focus. Evades antibodies by infection and vaccination.
BA.2.86 which is extremely close to JN.1, the variant taking the world by storm right now, and as I wrote last time, the virus is now trading growth, for persistence, therefore it may increase disease severity (slowly…but surely). It takes a lot more of the virus to get into the lung, which can hinder its transmissibility (trading growth for persistence).
Repeating myself, we are relying heavily on our T-Cells to do the heavy lifting, and Omicron variants already found a way to affect that to different degrees, since mutating the “lego pieces” the T-Cells prefer is very hard from an evolutionary perspective right now. Given the mix-and-match of immune responses and the idiocy of eternal boosting, if the virus ever does change the lego pieces, we are in for a wild ride.
Besides the long-term sequelae, this is actively my main concern and has been since the last quarter of 2022. Some of my lingering questions remain.
How effectively can all these new variants use all the other receptors SARS-CoV-2 is able to use, and if they all have similar effects as the primary strains.
FYI, there is only one, effective from my experience if allied with other supplements, TMPRSS2 inhibitor. Bromhexine and it is not the first time I have mentioned it. Prescription-only in the US, not illegal to import. As a medical YouTuber I like says.
“Take care of yourself and be well.”
If you chose to support this work, or supported at any time, in any form, thank you =) !
Next article may take a little longer to publish, I will try find a way to leave a simplified summary there, it won't be super complex, but the one after that may induce a headache on some of you.
Unrelated to anything I ever wrote about. Just out of pure curiosity, does any of my readers play Magic The Gathering ?
I wish everyone a great rest of the week ahead.
Bravo!! "My goal here is not to feed the doom and gloom hamster wheel of attention that moves society now but to bring awareness."
Here we are. We need to understand, as much as possible, what is happening and how to prepare for sad and difficult times. Find your people who are centered and balanced, avoid the emotion. It's draining.