


Covid effects in the pediatric brain
And the changes in other pathogens

Given not only the mounting evidence, but the number of signals one can observe via Real-World Data Analysis on the decline of cognitive function en masse, here is a reminder. I have long stated that Long Covid can be used as an unorthodox forecasting tool when it comes to the long-term damage any form of SARS-CoV-2 can induce, at a substantial amount of the global or national population.
Affecting 15% to 20% of a given country's workforce is absurdly catastrophic over any meaningful period of time, and here it does not matter whether blue or white-collar jobs are being affected. That country is still facing a significant gap in the decline of productivity and an increasing healthcare burden. Something that I and others predicted in early 2021.
Barely a week ago, I wrote about a very interesting paper on lasting Glymphatic dysfunction in Long Covid patients. To recap, a subgroup of Long Covid patients, mostly who suffer from neurological symptoms, have “defective” glymphatic function, which in turn makes the brain unable to “clean itself”, and allows low-grade neuroinflammation to last, perpetuating the dysfunction.
In said patients, the body attempts to compensate, although to an unsatisfactory degree, and the part most affected is the Left Hemisphere of the brain, responsible for Language, complex tasks, and low and high-order mathematics.

The following study comes from China, which has 0 mRNA in sight.
Multimodal MRI analysis of COVID-19 effects on pediatric brain
In a broader and simplistic sense, we have data on the neurological impact of different levels of SARS-CoV-2 infection in many age groups, but we sorely lack data both short and long-term of the impact of mild infections in children, we do know they have a distinct immune response from even adolescents, let alone adults, but if a mild infection already impacts the adult brain, be it without or with (Long Covid) sequelae, how does a mild infection affects a developing brain ?
That is exactly the question the authors wish to clarify. Here they chose 19 children between the ages of 1-6 years who were diagnosed with mild Covid infection, and were at least 2 weeks post-recovery, they excluded any children with prior neurological conditions or developmental ones. 22 healthy children were chosen as controls. They were recruited between February 2023 and May 2023, thus, the dominant variant was Omicron (likely) XBB.
Cortical Thickness metrics
Cortical tests measure the brain’s outer layer, its area, and volume (the amount of gray matter), and LGI, which stands for Local Gyrification Index, it measures how complex the folding in a localized region is, more folding indicates greater complexity. Statistical comparison between both groups demonstrated increased cortical thickness in the left lateral occipital cortex, and in the left superior parietal cortex, they found increased surface area, volume, and LGI.
Finding these structural differences, they wanted to investigate how brain regions connect and organize into networks. They assessed global and nodal network parameters. Global network parameters measure the overall organization of the brain network, with one of the main measurements being Cp (Clustering Coefficient), which reflects the tendency for connected regions neighbors to also be connected to each other. Nodal network measures the role and importance of individual brain regions (nodes) within the network, identifying critical communication "hubs."
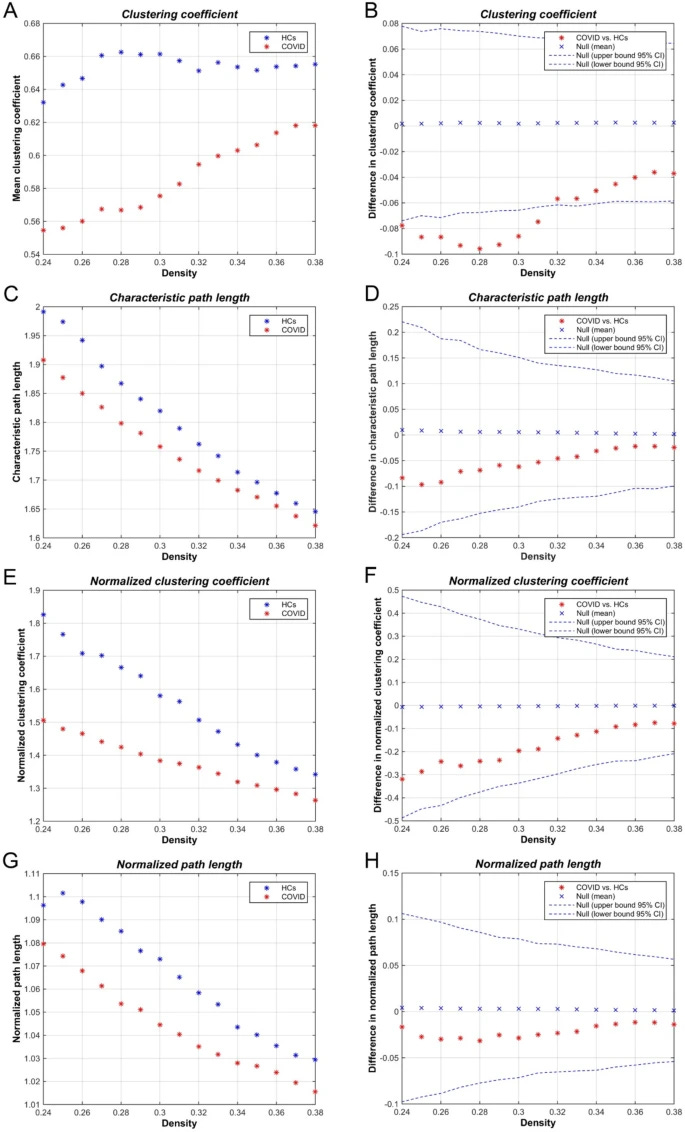
Compared to healthy children, children recovered from a mild Covid infection had lower Cp, suggesting reduced local interconnectivity, meaning less tightly clustered, thus losing efficiency in processing information. In the nodal network testing, they found an alteration, a shift in the location and number of critical communication hubs.
In healthy controls, hubs were found in areas like the precuneus and frontal cortex, regions crucial for complex thought, self-awareness, and executive function. In the Covid-recovered children group, these integrative hubs were less prominent, with the remaining hubs being located primarily in the sensory and motor areas.
This shift means the brain structure in children post-Covid is less centered around key regions responsible for complex thought and integration, and they become more centered around basic sensory and motor areas. Effectively, it means a reduction in the efficiency of higher-order cognitive processing. It's as if their brains might be prioritizing essential functions over more complex integration tasks, possibly as a response to subtle, widespread effects of the infection or inflammation.
The Brain's Waste Clearance: Glymphatic System
Their last test is one test readers might be familiar with. DTI-ALPS, which uses diffusion MRI to infer how efficiently water moves along perivascular spaces, a pathway for CSF flushing out waste. They also measured the volume of the CP (Choroid Plexus), the structure within the brain's ventricles that primarily produces CSF, the very fluid the glymphatic system relies on.
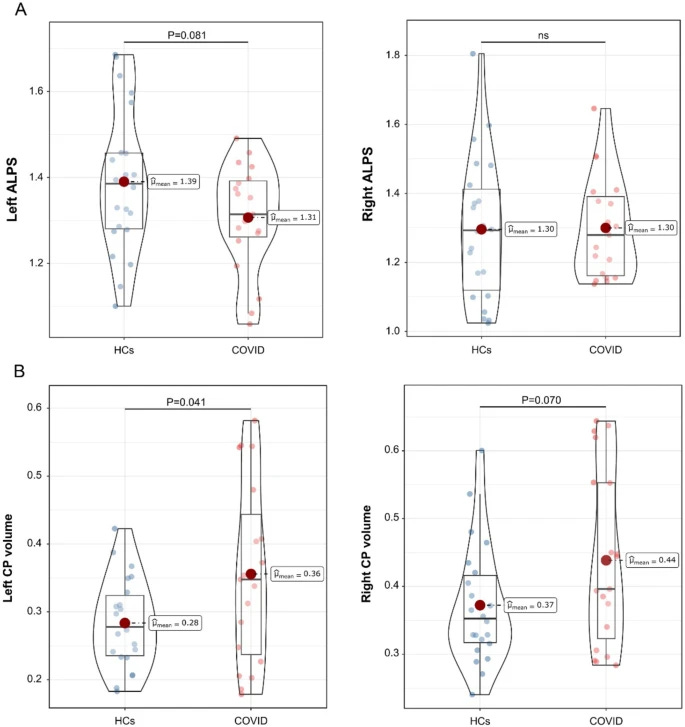
They observed increased volume, which indicates either inflammation or altered CSF production. There was a trend towards lower DTI-ALPS in the left hemisphere of the Covid children, but it didn’t reach statistical significance. If this test is done with the same children at 6 and then 12 months later, I would expect changes to this, if findings in adults serve as any indication.
These findings implicated something distinct from other papers we have covered, children with mild Covid have increased cortical metrics in specific regions, in contrast to what we see in adults, which is atrophy, loss. This can indicate their bodies are compensating and relying on plasticity. But it also shows us there is neuroinflammation going on, even after the infection clears, affecting the glymphatic system itself.
A similar loss as adults in efficient processing (how the brain connects), waste clearance failure (how efficiently the brain cleans itself from misfolded proteins and general waste), and impairment in higher-order cognitive integration. The most striking and intriguing part is that, once again, similar to all other age groups, the most impacted side of the brain was the Left Hemisphere, which is the side in children with impaired glymphatic dysfunction, albeit not as drastic as adults.
Given that we are talking about children, I will take the opportunity to also share something else. Related to an earlier article.

Co-detection of various viruses in SARS-CoV-2 in children with respiratory infections
The co-detection of SARS-CoV-2 variant with other respiratory virus has been extensively investigated. However, conclusive evidence remains elusive and conflicted. This study investigated the source- and age-dependent prevalence, incidence, and co-detection of multiple viral infections in children younger than 18 years old who presented with clinical symptoms indicative of respiratory infections during SARS-CoV-2 pandemic. We retrospectively obtained and analyzed pediatric patients admitted to the institution and underwent Film Array Respiratory Panel (BIOFIRE® RP2.1) testing between January 2021 and December 2022. This encompassed pre-Delta, Delta and omicron periods, evaluating Film Array results for singular and co-detections. The overall detection rate was 84.2% (1670/1983) among 1,983 pediatric patients. Of these, 106 were SARS-CoV-2 positive. Notably, 45 patients (42%) harbored SARS-CoV-2 as the sole pathogen. Co-detection was significant; 32 cases (30.2%) involved Human Rhinovirus/Enterovirus, 29 (24.5%) involved parainfluenza 3, and 26 (24.5%) involved Respiratory syncytial virus. Peaks of co-detected parainfluenza 3 and Respiratory syncytial virus were evident in the winter of 2022 and absent in 2021. The top three viral strain for co-detection was HRV/EV, PIV-3, and RSV. The emergence order of co-detection strain was HRV/EV ◊PIV-3◊ RSV during the Omicron period in Taiwan. We identified characteristic patterns of SARS-CoV-2-associated co-detections, with a notable emphasis on the co-detection of HRV/EV, PIV3, and RSV alongside SARS-CoV-2. This association appears to hold heightened significance during the Omicron variant era compared to earlier SARS-CoV-2 variants, which contrast with previous studies. The simultaneous circulation of different variants may contribute to variations in viral co-detection, particularly in young children, warranting further investigation.
During the early days of the pandemic, many common, seasonal viruses suddenly vanished, and conclusive proof of the mechanisms behind this is lacking, some attribute it to viral interference, when one specific virus takes over so aggressively, it displaces others, outcompeting them. Others attribute it to the restrictive measures, such as masks (lol, lmao even), social distancing, and the lockdowns (these 100% affect the patterns of many pathogens).
Regardless, at the tail end of 2021, changes in seasonality and patterns could be observed via signals on social media and clinical observation being shared. 2022, and especially 2023 onwards, the changes were drastic enough that even the media picked up.
Now we have more evidence on the changes of which pathogen was active during each year, they follow seasonal patterns (although some are displaced from their precise pattern), but more interesting to me, how Omicron differs from the rest and how it affected co-infections and other pathogen’s behaviors.
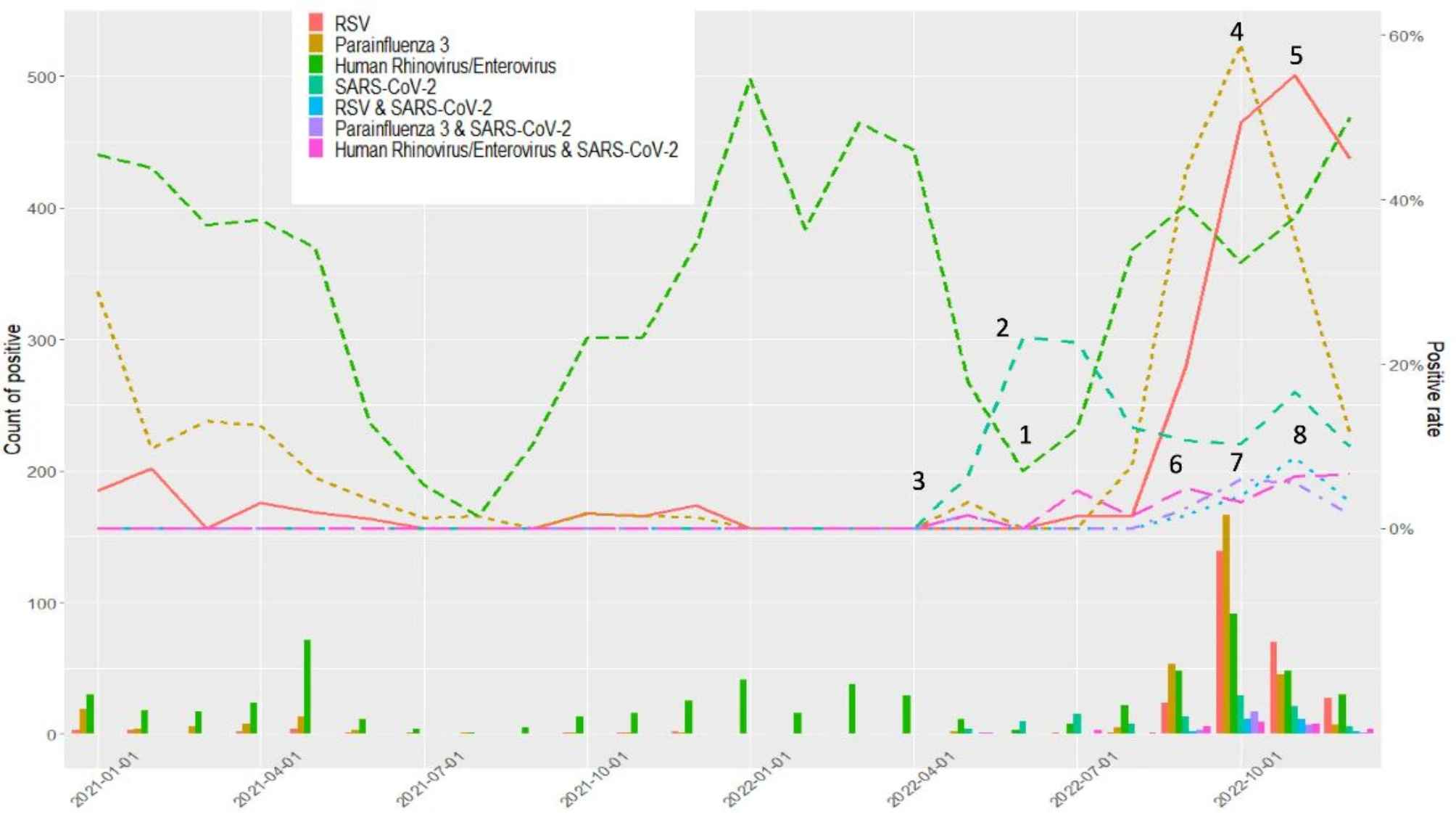
Here the authors found an “odd” trend, where before the arise of Omicron, the co-detection of SARS-CoV-2 with other pathogens, in this case HRV/EV, PIV3 (Parainfluenza), and RSV was rarely observed. There is a significant interplay between being infected with SARS-CoV-2, and weeks down the line, you get an infection with another pathogen, while your immune system is still recovering from the first exposure.
You can clearly see it in the graph below, where weeks after Omicron peaks, it declines but doesn’t vanish, HRV/EV, PIV3, RSV surge, at different time points. Co-detection is as important as co-infection, because Omicron creates a whole distinct cascade on its own, and makes every age group susceptible to other infections over a long enough period.
Each of these pathogens can contribute to specific long-term changes that remain statistically a blip, or even misinterpreted as noise, until significant pressure in the healthcare system, or retroactively looking at the data points towards otherwise. Over the years, I have brought to attention specific non-linear dynamics that came to be observed by clinicians and researchers globally 6-12 months later, and this has more importance than some attribute.
I thought about writing something additional here, but I will leave this article as it is. I will leave you with some form of good news, as I go play video games to take care of cognition. Was this a joke ?
Associations of computer gaming with incident dementia, cognitive functions, and brain structure: a prospective cohort study and Mendelian randomization analysis
Methods
We included 471,346 White British participants without dementia at baseline based on the UK Biobank, and followed them until November 2022. We estimated the risk of dementia using Cox proportional hazard models, and assessed the changes of cognitive functions and brain structural measures using logistic regression models and linear regression models. Mendelian randomization (MR) analyses were performed to examine the association between genetically determined computer gaming and dementia.
Results
High frequency of playing computer games was associated with decreased risk of incident dementia (HR, 0.81 [95% CI: 0.69, 0.94]). Individuals with high frequency of playing computer games had better performance in prospective memory (OR, 1.46 [1.26, 1.70]), reaction time (beta, -0.195 [-0.243, -0.147]), fluid intelligence (0.334 [0.286, 0.382]), numeric memory (0.107 [0.047, 0.166]), incorrect pairs matching (-0.253 [-0.302, -0.203]), and high volume of gray matter in hippocampus (0.078 [0.023, 0.134]). Genetically determined high frequency of playing computer games was associated with a low risk of dementia (OR, 0.37 [0.15, 0.91]).
Conclusions
Computer gaming was associated with a decreased risk of dementia, favorable cognitive function, and better brain structure, suggesting that computer gaming could modulate cognitive function and may be a promising target for dementia prevention.
Computer gaming lowers your dementia risk, favors better cognitive function, and even affects, positively affects the brain structure. Depending on the study you decide to read, they demonstrated positive impacts, such as certain studies demonstrating that those who play video games have better verbal working memory, visuosptial working memory, processing speed, and attention.
Different genres will positively impact the brain in unique manners. Everything in excess is bad, but playing games a few hours a week may be the most beneficial intervention for most people. I guess it wasn’t a joke.
I am grateful for your continued support, and if you decide to become one, thank you too !

It was actually a joke lol. A serious question now.
Do my readers prefer the Cognitive Strike Part III being one, MASSIVE article, or just a bunch of not short, but not long articles covering the papers in said article (there are quite a few) ?
Without your input, I will just write a massive one.
It’s pretty depressing to read these articles, I often either wish I didn’t read the ones about kids or I want to kill myself afterward. But I’m proud of you for covering it because is few people will. I’ve spent a year and change trying to come up with a protocol for kids which I’m comfortable with and I’ve finally done it but I’m afraid to share anything for kids with anybody but my closest friends. And most of them don’t really care about covid or vax anyway. I do worry about their brain function but my big hope is thr plasticity is more in a growing brain so in time they can potentially repair. Luckily Taurine is suitable for kids in small doses as is Choline so there are supplements out there to help