
Biological Briefing
Mimics all around.

Undecided on the format, the frequency, etc. I expect a good amount of times will be me, commenting on tha papers or referring to shit I said months ago. Like this one.
Months ago, on the memetic train of Fleming set off a viral meme upon the minds of untold hundreds of thousands. The SARS-CoV-2 Prion bullshit, and other two specially moronic people with very little understanding of cell biology or medicine spread it far and wide (Walter Chestnut, and Adam “Very Virology”).
Besides other points, I argued that the way they presented it (they didn’t even present a pathway or mechanism, they don't know which proteins are being up or down regulated, where the proteins are coming from, how the fibrils are being formed, in response to what) was NOT how prion diseases would occur in people infected or vaccinated. Among various mechanism, I said the main one was mitocondrial dysfunction (the literature is pretty clear), the accumulation of ROS inside the cells in the brain, and expression of specific cytokines and factors.
So you don’t waste time, there are simple and effective ways to deal with this. One of the most common ways mitochondrial dysfunction happens, and therefore the set off or worsening of neurologic diseases, is by the depletion of both extra and intra-cellular Glutathione (among other mechanisms).
The fact that both the dead virus and the spike alone cause MD is concerning, bear weight to one of my insane ideas.
Mitochondrial Dysfunction: A Prelude to Neuropathogenesis of SARS-CoV-2
The SARS-CoV-2 virus is notorious for its neuroinvasive capability, causing multiple neurological conditions. The neuropathology of SARS-CoV-2 is increasingly attributed to mitochondrial dysfunction of brain microglia cells. However, the changes in biochemical content of mitochondria that drive the progression of neuro-COVID remain poorly understood. Here we introduce a Raman microspectrometry approach that enables the molecular profiling of single cellular organelles to characterize the mitochondrial molecular makeup in the infected microglia cells. We found that microglia treated with either spike protein or heat-inactivated SARS-CoV-2 trigger a dramatic reduction in mtDNA content and an increase in phospholipid saturation levels. At the same time, no significant changes were detected in Golgi apparatus and in lipid droplets, the organelles that accommodate biogenesis and storage of lipids. We hypothesize that transformations in mitochondria are caused by increased synthesis of reactive oxygen species in these organelles. Our findings call for the development of mitochondria-targeted therapeutic approaches to limit neuropathology associated with SARS-CoV-2.
Endogenous Deficiency of Glutathione as the Most Likely Cause of Serious Manifestations and Death in COVID-19 Patients
Higher rates of serious illness and death from coronavirus SARS-CoV-2 (COVID-19) infection among older people and those who have comorbidities suggest that age- and disease-related biological processes make such individuals more sensitive to environmental stress factors including infectious agents like coronavirus SARS-CoV-2. Specifically, impaired redox homeostasis and associated oxidative stress appear to be important biological processes that may account for increased individual susceptibility to diverse environmental insults. The aim of this Viewpoint is to justify (1) the crucial roles of glutathione in determining individual responsiveness to COVID-19 infection and disease pathogenesis and (2) the feasibility of using glutathione as a means for the treatment and prevention of COVID-19 illness. The hypothesis that glutathione deficiency is the most plausible explanation for serious manifestation and death in COVID-19 patients was proposed on the basis of an exhaustive literature analysis and observations. The hypothesis unravels the mysteries of epidemiological data on the risk factors determining serious manifestations of COVID-19 infection and the high risk of death and opens real opportunities for effective treatment and prevention of the disease.

One of the most common deficiencies in most people is Magnesium, also one of the factors that drive the severity of the disease, and I personally believe might affect the immuno supression and at a minor scale the autoimmunity.
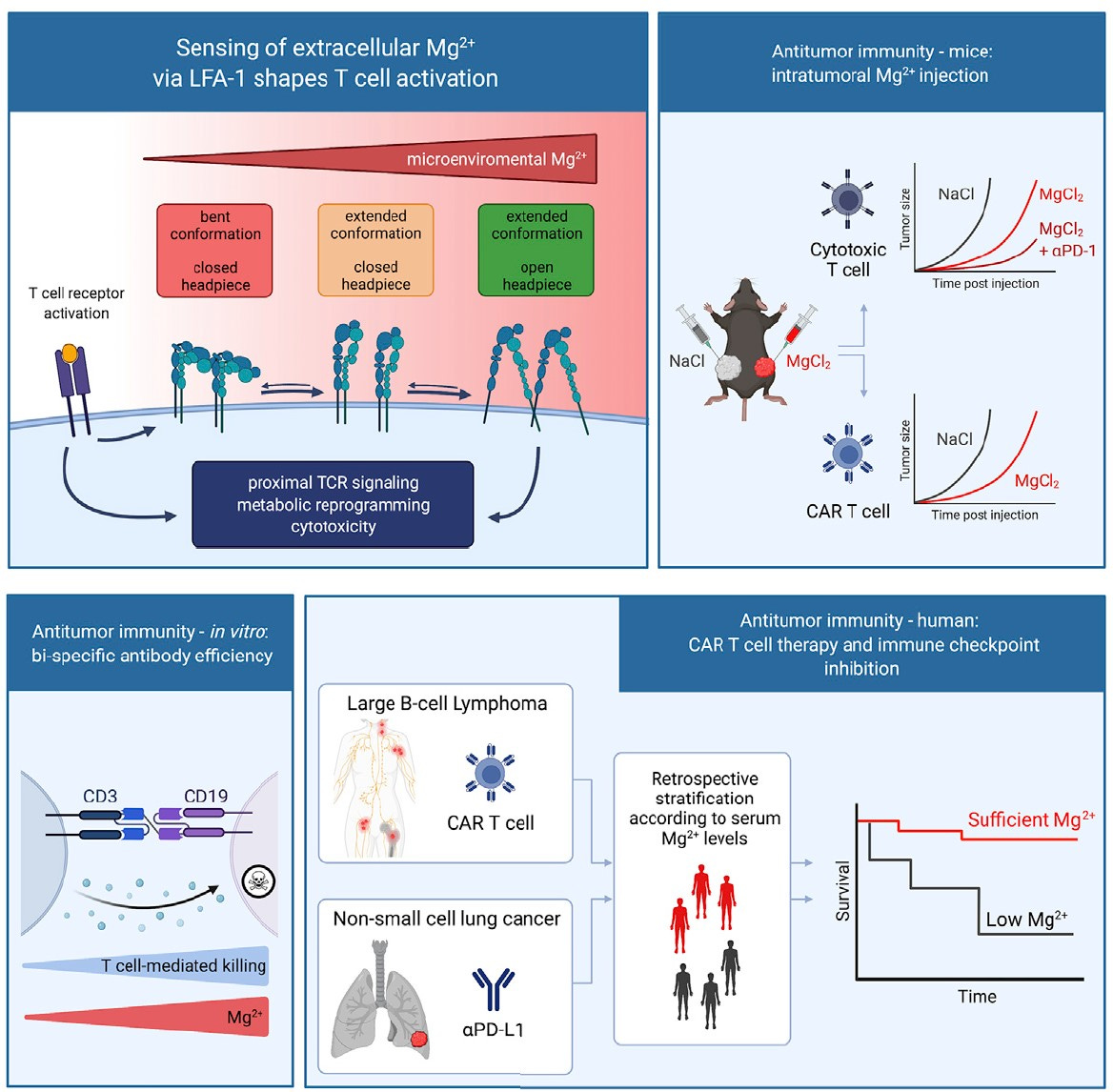
Magnesium Enables Immune Cells to Tackle Infections and Cancer
Through a study that adopts approaches ranging from structural biology and basic biochemical assays to preclinical immunology and clinical research, Hess and his team show magnesium is important for the functioning of a cell surface protein on CD8+ T cells called leukocyte function-associated antigen 1 (LFA-1). The findings are published in a January 19 article in the journal Cell titled, “Magnesium sensing via LFA 1 regulates CD8+ T cell effector function.”
Someone asked me my opinion on the paper Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations: The role of G-quadruplexes, exosomes and microRNAs. Some of you may not like my opinions.
The only parts of some validity for me are 9 and 10, and the TLR the rest is the usual academic way of writing papers. You fill it to the brim with references to make it sound much, much more plausible. The paper itself is good, and into a good direction but it lacks what someone way smarter than me hammered inside my head.
What are the pathways and how upstream you can go ?
Read all my Plagued by Design posts and the Reverse AIDS hypothesis, all merely introductions to Part II (undecided if I am going to write it or not). The don’t even cite the most important cytokines, the integrin activation, the excessive expression of certain Interleukin, the mimicry of the spike to SEB, it’s antigen mimicry. What about the mimicry of insulin ? They didn’t even mention one of the drivers of turbo charging so many of the cancers, autoimmunity and thyroid issues, one of the papers they cite did (it’s a Interferon). I also have a intellectual gripe with Stephanie, because she too was on the prion bullshit train. And after months, in a podcast, finally saw some light and reached the conclusion based on evidence.
Which is don’t take more than 2 injections, and supply your body with enough antioxidants and specially glutathione, and 99.95% of people will be fine. Don’t get me wrong, I called the pathways we unconvered as Hermesian Pathological Pathways for a reason. Hermes the God of Speed. Because both jab to a insane degree and virus to a lesser degree are disease accelerators.
Would like to leave this paper here if I write the second part of Reverse AIDS, or you want to dig into Toll Like Receptor.
COVID-19 and Influenza coinfection: The rise of Ômicron and H3N2 in Brazil - 2022
This is also a very important one, since the start of the pandemic, mimicking the Spanish Flu, what kills most severe patients besides the immune dysregulation, is the secondary infections. Again, TLR will come to play.
Researchers report 21% COVID-19 co-infection rate
And for last, hammering my mimicry point.
Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins With Tissue Antigens: Implications for Autoimmune Diseases
We found that SARS-CoV-2 antibodies had reactions with 28 out of 55 tissue antigens, representing a diversity of tissue groups that included barrier proteins, gastrointestinal, thyroid and neural tissues, and more. We also did selective epitope mapping using BLAST and showed similarities and homology between spike, nucleoprotein, and many other SARS-CoV-2 proteins with the human tissue antigens mitochondria M2, F-actin and TPO. This extensive immune cross-reactivity between SARS-CoV-2 antibodies and different antigen groups may play a role in the multi-system disease process of COVID-19, influence the severity of the disease, precipitate the onset of autoimmunity in susceptible subgroups, and
We sought to determine whether immune reactivity occurs between anti-SARS-CoV-2 protein antibodies and human tissue antigens, and whether molecular mimicry between COVID-19 viral proteins and human tissues could be the cause. We applied both human monoclonal anti-SARS-Cov-2 antibodies (spike protein, nucleoprotein) and rabbit polyclonal anti-SARS-Cov-2 antibodies (envelope protein, membrane protein) to 55 different tissue antigens. We found that SARS-CoV-2 antibodies had reactions with 28 out of 55 tissue antigens, representing a diversity of tissue groups that included barrier proteins, gastrointestinal, thyroid and neural tissues, and more. We also did selective epitope mapping using BLAST and showed similarities and homology between spike, nucleoprotein, and many other SARS-CoV-2 proteins with the human tissue antigens mitochondria M2, F-actin and TPO. This extensive immune cross-reactivity between SARS-CoV-2 antibodies and different antigen groups may play a role in the multi-system disease process of COVID-19, influence the severity of the disease, precipitate the onset of autoimmunity in susceptible subgroups, and potentially exacerbate autoimmunity in subjects that have pre-existing autoimmune diseases. Very recently, human monoclonal antibodies were approved for use on patients with COVID-19. The human monoclonal antibodies used in this study are almost identical with these approved antibodies. Thus, our results can establish the potential risk for autoimmunity and multi-system disorders with COVID-19 that may come from cross-reactivity between our own human tissues and this dreaded virus…
Another concern from molecular mimicry is the potential role it may play in vaccine safety. Several incidences of viral infection and vaccine-induced autoimmunity specific to cross-reactivity have been reported in the literature (8). In 2009, the vaccines developed to treat the H1N1 pandemic lead to narcolepsy specifically due to cross-reactivity. The inactivated split-viron particles (ASO3) shared cross-reactive homology with hypocrites found in theypothalamus, leading to selective destruction of that substance after vaccination in a subgroup of susceptible individuals (13). Vaccination with ASO3 lead to a three-fold increase in the onset of narcolepsy compared to individuals who were not vaccinated (61).
During the swine flu outbreak in the late 1970s in the United States, the use of influenza vaccination was found to induce a four- to eight-fold increased risk of developing Guillain-Barré syndrome due to cross-reactivity (14). Cross-reactive relationships between viral infections and vaccinations have also been found with hepatitis B and myelin proteins leading to multiple sclerosis, human papillomavirus and nuclear proteins leading to systemic lupus erythematosus (SLE), coxsackievirus and islet cells proteins leading to type 1 diabetes, etc (15–18). Razim et al (62)., in designing a vaccine against Clostridium difficile, concluded that before considering a protein as a vaccine antigen, special care should be taken to analyze and remove the sequences of tissue cross-reactive epitopes in order to avoid possible future side effects.
‘When I Told Pfizer About Incidents of Myocarditis They Refused to Believe Me for Four Months’
Israel had the potential to be the first country in the world to detect side effects of the coronavirus vaccines. And it did detect two, almost by accident. But its disregard for more minor effects cost it public trust
Imagine the cancers, autoimmunity and neurodegeneration. Maybe when we have 300 million chronically ill patients around the world, Pfizer and goverments may accept, some though, are already seeing the writting on the wall.

*If you like or take some value of my posts, feel free to support me, most of it will always be free. And I invest more time doing this full time and getting better, creating better content.
One friend got his thyroid removed completely after they discovered an anomaly. I didn't want to ask too much what was the diagnosis as he looks pretty destroyed. Definitely not that taking 2 pfizer was probably the cause.