
Bio Briefing - Reverse Transcription, Omicron, and bad vaccine efficacy
One molecule to rule them all.

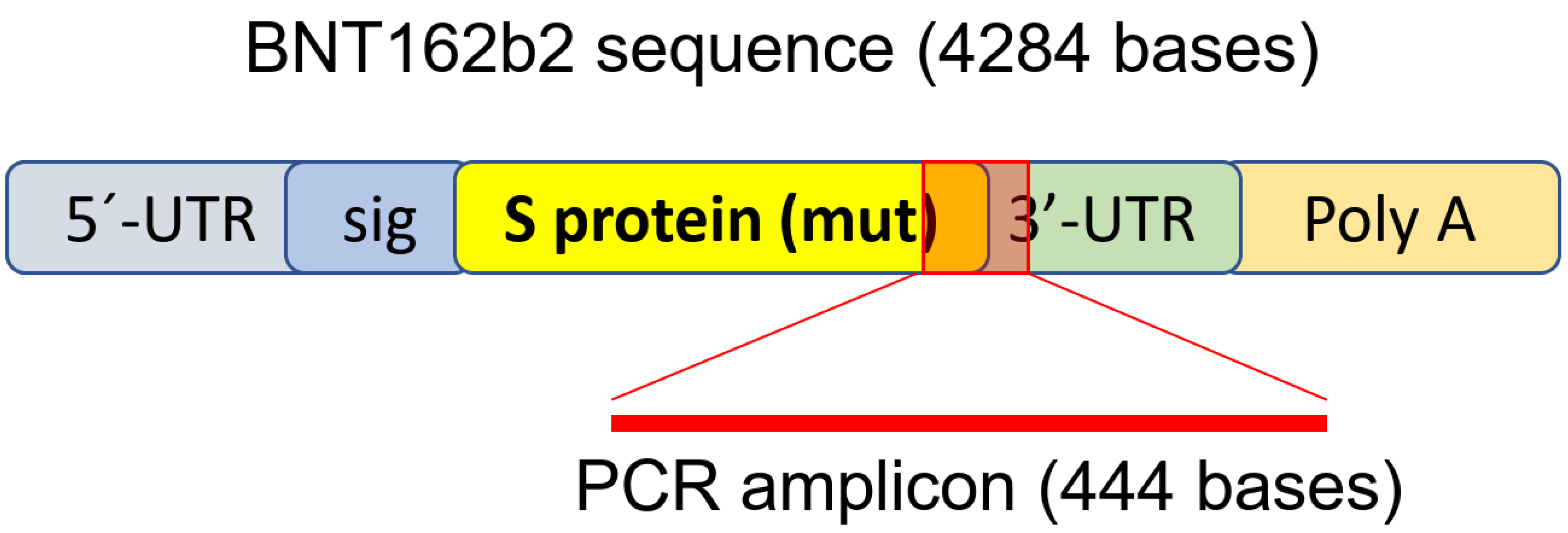
The paper everyone is talking about can be found here. The title is Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line.
This paper has a lot to unpack, Igor here on Substack already cover parts of the paper, so you should read it, here I will do the usual. The whole, the system, the hidden complexity.

A lot to unpack here. Bear in mind, this is a cell line study, and not a in vivo (a living being) one. It is still significant. The vaccine mRNA is quickly up taken into the liver cell and are reverse transcribed inside the cell into DNA in 6 hours. R/T does not mean it was integrated into your damn genome.
But it doesn’t mean the local cells will start producing the payload (the Spike Protein), and nobody knows for how long. Now is a good time to read my post (Insert the germinal center paper here).
Furthermore, in animals that received the BNT162b2 injection, reversible hepatic effects were observed, including enlarged liver, vacuolation, increased gamma glutamyl transferase (γGT) levels, and increased levels of aspartate transaminase (AST) and alkaline phosphatase (ALP) [26]. Transient hepatic effects induced by LNP delivery systems have been reported previously [27,28,29,30], nevertheless, it has also been shown that the empty LNP without modRNA alone does not introduce any significant liver injury [27]. Therefore, in this study, we aim to examine the effect of BNT162b2 on a human liver cell line in vitro and investigate if BNT162b2 can be reverse transcribed into DNA through endogenous mechanisms.
At the very least, this paragraphs demonstrates by using previous evidence, that the LNP alone don’t cause any measurable changes in the liver, alas the mRNA infection (mRNA+LNP) does cause liver damage. Even though the damage is reversible, following the entire paper, this is just the initial damage, and everything else compounding.
One thing few mention, that part in red is the part they measured, not the entire sequence.
I have problems with this entire paper, first the cell line used, it is a cancer cell line, that will affect the results, second is the section they used, and not the entire S protein, but I do think the findings might be of concern. The biggest find is the higher expression of LINE-1. LINE-1 is now a good used a cancer marker, here good papers about it, 1, 2, 3.
The cell line used is from a Japanese cancer patient suffering from liver cancer, this will impact the overall design of the experiment, they didn’test these in KO (meaning without) LINE 1, well, anything. This alone would prove that LINE 1 is the thing responsible for the Reverse Transcription.
Let us assume, then, that this might actually happen (as a friend said, the paper is ambiguous, and another the paper leaves too much in the air) this happens in a transient (of short duration) manner. This raises the point I did it before.
Does presence of mRNA in Germinal Centers make your cells express the Spike protein for X amount of time, basically a continuous antigen presentation, which will lead to a cascade of physiological damage. The same principle would be applied here, the present of the part they test, or worse, transcription would mean continuous antigen presentation, which will lead to autoimmunity, and liver damage, and everything in between.
This can’t happen with natural infection, for the layman it is really hard, but for the scientific literate, design of study matters. A lot. Yet for me, the biggest find was the expression and production of Spike protein in the liver. Why ? Two reasons.
Amylin. If you search for SARS-CoV-2 Serum Amyloid A, you will find this protein is highly expressed among many of the infected, it is a driver of disease, but the real driver of long term damage is Amylin. A hormone, it’s accumulation (or high expression) in the liver will lead to both Type 1 and 2 Diabetes using different immune pathways, and high concentrations in the blood will lead, among o other things, neurodegenration.
Protein mimicry. Which this virus is filled with. And, in certain condition, and genetic predisposition, it will set off diabetes at scale.
Further research upon what these authors found, and a better designed study should be done ASAP.
And just for laughs, and the memes, Chile just passed a law that guarantees the rights of genetically modified humans.
Omicron BA.1 and BA.2 are antigenically distinct SARS-CoV-2 variants
I find this entire paper contrived on the authors findings, yet a few nuggets of gold here and there.

Something I have already commented before, Omicron BA. 2 differs significantlly to BA.1, and it is coming to dominate several highly vaccinated countries, at least in the abstract the authors mention both variants escape vaccine-induced antibody response.
Many said BA.1 (what was referred to Omicron for many weeks) did not blast through immunity acquired by previous infection, which is clearly at the very least a misconception, that is why you should always assess the information, and wait for further evidence. I found very curious that you get different post vaccination, you got different response to BA. 1 and BA. 2.
Given a little more evidence that they are antigenically different, therefore elicit different immune response, and thus cause different degrees of disease. By no means this shows greater severity, that would need another research entirely.
Where I completely disagree, and any layperson with a ounce of common sense would be able to pick up too is the follow, repeat exposure to the original original antigen can increase your protection. Yeah, but at what cost (antigenic drift, mutations, new variants, and low protection… how someone write this paper and that phrase…).

Again, authors mention both BA. 1 and BA. 2 escape vaccine induced immunity, and try to say population immunity is exerting selective pressure on SARS-CoV-2. No, not population immunity, crap vaccine elicited immunity is creating antigenic distinct variants.
If anything, most researchers, and even Bill Gates accept Omicron gives a better immunity to naive (never infected), and a broader immunity to the previous infected.
I agree that, given the pandemic didn’t end, and the dominance of all forms of Omicron derived variants, we will see more re-infections, which is bad in my opinion. This isn’t the flu, regardless of how much changes were achieved in the Omicron proteins, it is still SARS. It will still accelerate disease in many, specially the vaccinated, and there is a chance of recombination, or just evolution shifting this into a more pathogenic variant.
Given more evidence to my point on crap vaccines.
Waning Effectiveness of the Third Dose of the BNT162b2 mRNA COVID-19 Vaccine
By conducting a retrospective study implementing a test-negative case-control design, analyzing 546,924 PCR tests performed throughout January 2022 by 389,265 persons who received three doses of the vaccine, we found that the effectiveness in each month since vaccination decreased significantly. Compared to those vaccinated early, on August 2021, relative protection against infection waned from 53.4% a month after vaccination to 16.5% three months after vaccination. These results suggest that there is a significant waning of vaccine effectiveness against the Omicron variant of the third dose of the BNT162b2 vaccine within a few months after administration
There are no snarky comments to be made, besides this is creating more problems, than helping any vaccinated person, and fueling new variants. The vaccines never worked, never would, and never will with Omicron and new lineages/variants. There is now a deluge of papers trying to manipulate the data by shady design study and modelling to push “vaccines work and save lives better than natural infection”.
I don’t have the time to debunk each other, or the will, so be aware this will be pushed HARD for months to come. Like this bullshit paper stating vaccination reduces your chance to develop Long Covid, yet I previously shared a paper that after two doses of vaccine, if you have a breakthrough infection, you have a sizable chance to develop LC, let alone the post-vaccination Long Covid like syndrome.
Another example, from this paper.
COVID19 vaccines protect from symptomatic infection by significantly reducing the risk of ICU hospitalization for severe disease. However, it seems they have trend to decrease their fully protection against SARS-COV-2 after five months regardless age, sex or type of vaccine.
At the end, the push a third dose, but also the ICU is a blatant lie, since every government in the planet is now hiding data, given the clear signs of what I called Reverse Marek. There are signs of ADE everywhere.
In the same post about Long Covid, A Case for Reverse Marek III, I posted and postulated about how the vaccinated individual can not build a (measurable) immunity against the N protein of SARS-CoV-2. And researchers just found that…
A role for Nucleocapsid-specific antibody function in Covid-19 Convalescent plasma therapy
We found CCP had the greatest clinical benefit in participants with low pre-existing anti-SARS-CoV-2 antibody function, rather than S or N antibody levels or participant demographic features. Further, CCP induced immunomodulatory changes to recipient humoral profiles persisted for at least two months, marked by the selective evolution of anti-inflammatory Fc-glycan profiles and persistently expanded nucleocapsid-specific humoral immunity following CCP therapy. Together, our findings identify a novel mechanism of action of CCP, suggest optimal patient characteristics for CCP treatment, identify long-last immunomodulatory effects of CCP, and provide guidance for development of novel N-focused antibody therapeutics for severe COVID-19 hyperinflammation.
Treatment of patients with COVID-19 convalescent plasma (CCP) exerted great changes in immune responses and immunomodulated people with dysfunctional,low antibody responses. What did catch my eyes was the N part.
We found that CCP shifted immunodominance to SARS-CoV-2 by diminishing the S-focused evolution in exchange for expanded N-specific activity. The clinical benefit associated with this immunodominance shift suggests three major findings: 1) the importance of blunting the inflammatory S-targeted humoral response in severe COVID-19, 2) the critical role of clearing N-specific immune complexes, and 3) the anti-inflammatory effects on the S and N humoral response are long lasting.
This strongly argues that part of the therapeutic benefit of a polyclonal antibody therapy is its capacity for immunomodulation. For CCP treatment of hospitalized patients with COVID-19, this effect manifests as a dampening of the antibody-induced macrophage/monocyte hyperinflammatory host response acutely and possibly even months after the resolution of COVID-19 viremia.
Authors found that CCP shifted the immunodominance of hospitalized patients, by diminishing the inflammation caused by Spike protein and response to it, and expanded the N response. Not only they were able to blunt inflammatory responses, they gave months worth of humoral (what you actually want) N response in said patients.
Sadly they do not differentiate or even mention if these are vaccinated or not, and I think it would be of great value if CCP could create, even if for just 2-3 months, N responses in vaccinated individuals. Would also be interesting to see the effect of CCP in some Long Covid patients. Good news nonetheless.
As I mention on Twitter a few times, Omicron is a trade off, but in my opinion is a worth one, and here the layperson can make sense on how just one aminoacid change can impact the whole course of the disease in many.
Omicron and Alpha P680H block SARS-CoV2 spike protein from accessing cholinergic inflammatory pathway via α9-nAChR mitigating the risk of MIS-C
Sequence homology between neurotoxins and the site encompassing the furin cleavage site 680SPRRAR685 in the spike protein (S) of CoV2 suggested that this site could interact with nicotinic acetylcholine receptors (nAChRs). Molecular dynamics simulations confirm robust structural similarity between wild-type (WT) CoV2 and the binding motif of α-conotoxin to α9 nAChR, which is known to modulate IL-1β in immune cells. We show that the structural integrity of this binding motif is eliminated by Alpha P681H mutation, reemerged in Delta variant P681R, and disappeared again with Omicron N679H/P681H. Interactions between the toxin-mimic CoV2 motif and α9-nAChR are expected to trigger the release of pro-inflammatory cytokines an effect that is mollified by Alpha and Omicron. Clinical features of this interaction site are relevant because, contrary to most regions in the S protein, the furin binding site does not appear to trigger an immune response prior to cleavage, indicating that the cholinergic pathway should be activated in the respiratory tract and nasal mucosa where α9-nAChR co-localizes with the virus. The correlation of changes on this motif by the different variants closely matches the reported cases of Multisystem Inflammatory Syndrome in Children by the CDC, and predicts significant mitigation of MIS-C with the Omicron variant. Our findings strongly motivate further study of this cholinergic pathway as one source of the cytokine storm triggered by CoV2.
The abstract is self-explanatory, the specific amino acid sequence blunts the hyper inflammatory response in the virus. You know where this sequence located, or rather, do you want to know ? In, now, the well known Furin Cleavage Site, in fact, this is the exact place for the SEB toxin. And if you read my Reverse AIDS posts, you know the importance of said sequence.
The brunt of the damage, and shift of immune response of the other variants mostly came from here. Molecular changes are important. A couple changes, you go from hyper inflammation and possible ADE, to a bad flu (with possible long term consequences.
And while you were sleeping, and paying attention to the war in Ukraine.
A National Vaccine Pass Has Quietly Rolled Out – And Red States Are Getting On Board
While the United States government has not issued a federal digital vaccine pass, a national standard has nevertheless emerged. To date, 21 states, the District of Columbia and Puerto Rico offer accessibility to the SMART Health Card, a verifiable digital proof of vaccination developed through the Vaccination Credential Initiative (VCI), a global coalition of public and private stakeholders including Microsoft, Salesforce, Oracle, the Mayo Clinic and other health and tech heavyweights.
And very soon, at least four more states will be rolling out access to SMART Health Cards. “We've seen a notable uptick in states that have officially launched public portals where individuals can get verifiable vaccination credentials in the form of SMART Health Cards with a QR code,” says Dr. Brian Anderson, co-founder of the VCI and chief digital health physician at MITRE.
We are in for the long fight. Or rather, the Long Night.
If you enjoy or take value from my independent, interdisciplinary analysis, consider becoming a free or paying subscriber, my work is now fully support by the reader. Sharing also helps me tremendously. Appreciate all supporters.
Thank you for this - this is the first post I've read that has analyzed the structure of the study in terms of how to value its conclusions. I think Sweden is pretty impartial was a whole and appreciate them producing this study since many wouldn't have touched it but if the structure is flawed then its results are suspect.
I am very sad my friends, after reading Igor’s Moderna and Pfizer’s cancer gene insert. I am very sad for all the children and families. May God have mercy and show love to us and them and his wrath to those that earned it.