


Bio Briefing - Reverse Marek III
One small protein to ADE them all.

Since I got lots of new subscribers. Bio(logical) Briefings are like my other daily posts. It’s an overall view of either interesting trends or papers that came out recently. Sometimes it will fit a major trend, other times, they are just fascinating or important papers. This one fits a lot of the SARS-CoV-2 trends I have been covering.
Whatever is not under quotes is my commentary.
mRNA-1273 or mRNA-Omicron boost in vaccinated macaques elicits comparable B cell expansion, neutralizing antibodies and protection against Omicron
This also implies that neutralizing antibody titers at extended times after vaccination may not be a reliable surrogate either for vaccine efficacy in the lower airway or for predicting responses following a boost or infection as they may not reflect the recall capacity of the underlying memory B cell population
The observation that boosting with either mRNA-1273 or mRNA-Omicron resulted in the expansion of a similarly high frequency of cross-reactive B cells likely stems from the principle of original antigenic sin, otherwise termed antigenic imprinting, whereby prior immune memory is recalled by a related antigenic encounter
Eugyppius covered this paper in his Substack, I concur with his analysis. There is no point in using an Omicron-based vaccine at best, but the problem is we vaccinated most of the planet with a spike that doesn’t even exist anymore. And I will make a continuous case for a Reverse Marek and how any vaccination with Spike only is stupidity at best, monumental backfire at worse. As this shows you.
From this paper.

As per what I tried to describe in this post and in It’s viral Evolution Baby, the vaccinated can’t amount a good enough neutralizing response, they can’t even neutralize the spike protein, and only give the virus room for mutation by poor neutralization and selective pressure. As the paper shows, the Pfizer vaccine might not even be enough to protect the vaccinated against severe disease, which is the last pillar the narrative and governments are relying on. I sure as hope there are no more deleterious effects from being vaccinated.

Today’s data shows that 94% of the deaths today were people over 60; averaging out to 97% for the last 7 days or 89% for people over 70 (81% of deaths were among the jabbed in the last 7 days). Source

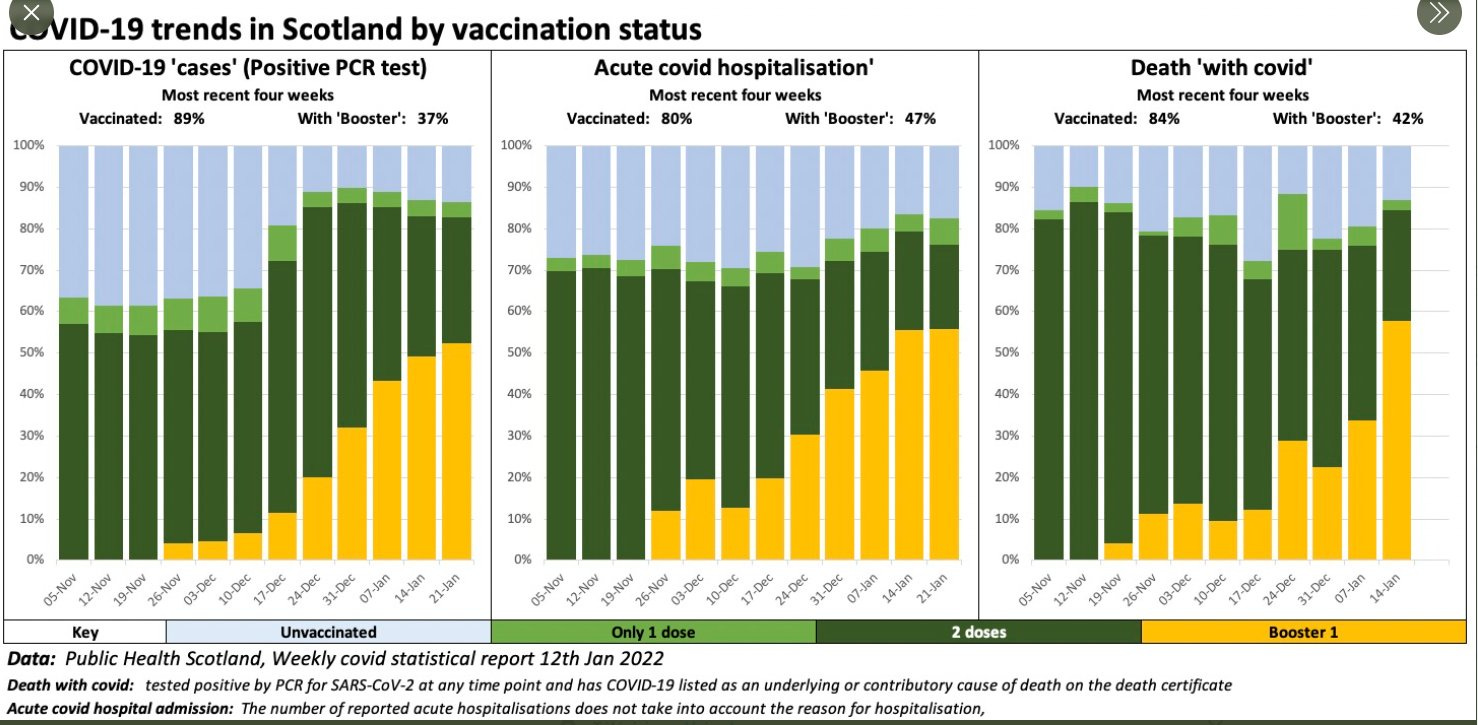
Scotland: unvaxxed 13% of covid deaths in the last week. 87% vaxxed. The most surprising is the rise of boosted, already 58% of deaths and growing.
COVID-19 (Coronavirus) statistics
05 February 2022
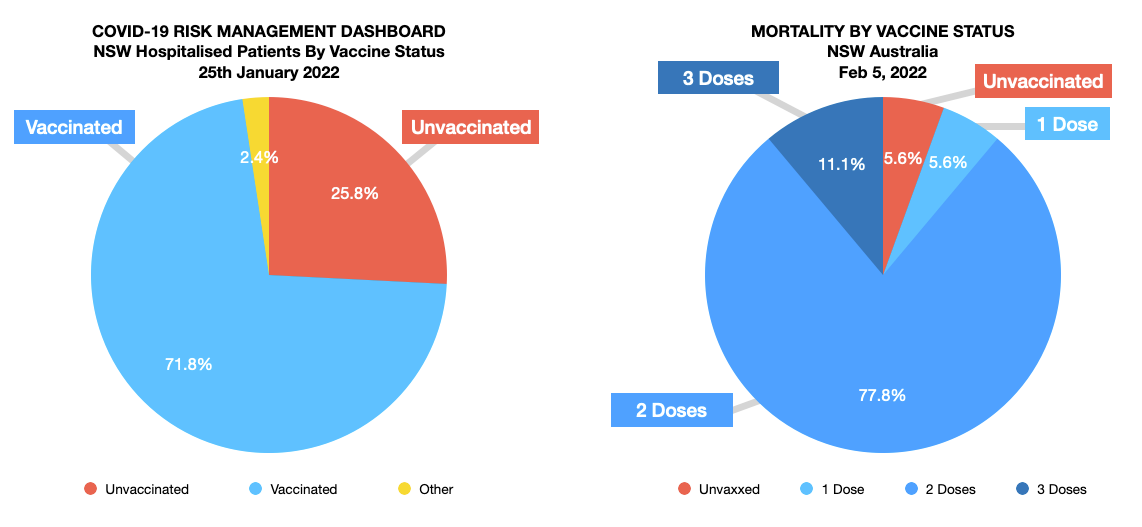
Across NSW, more than 95 per cent of people aged 16 and over have received a first dose of a COVID-19 vaccine, and 94.1 per cent have received two doses to Thursday 3 February 2022.
Two people who died were aged under 65, a woman and a man. Both had received two doses of a COVID-19 vaccine and one person had significant underlying health conditions.
Two people who died had received three doses of a COVID-19 vaccine, 14 people had received two doses, one person had received one dose, and one person was not vaccinated.
Prevalence, characteristics, and predictors of Long COVID among diagnosed cases of COVID-19
Prevalence of Long COVID among patients with mild/moderate disease (n = 415) was 23.4% (95% CI: 19.5%,27.7%) as compared to 62.5% (95% CI: 50.7%,73%) in severe/critical cases(n=72). The most common Long COVID symptom was fatigue (64.8%) followed by cough (32.4%). Statistically significant predictors of Long COVID were - Pre-existing medical conditions (Adjusted Odds ratio (aOR)=2.00, 95% CI: 1.16,3.44), having a more significant number of symptoms during acute phase of COVID-19 disease (aOR=11.24, 95% CI: 4.00,31.51), two doses of COVID-19 vaccination (aOR=2.32, 95% CI: 1.17,4.58), the severity of illness (aOR=5.71, 95% CI: 3.00,10.89) and being admitted to hospital (Odds ratio (OR)=3.89, 95% CI: 2.49,6.08).
One of the biggest risks for Long COVID is…. Two doses of vaccination. If you read all my virus posts, you can quite make sense of it.
When you don’t neutralize the spike, you have pieces of it floating around, and this is actually one of the (many) drivers of long COVID, all the protein mimicry and antigens from other fungi and bacteria stitched in a protein.
That will signal your body to produce specific inflammatory responses, which after a while the body will see as it is wrong, and try to correct it, leading to a cascade of constant inflammation for months and months. To understand the meaning of the tweet below, just read my A Stronger Case for Reverse Marek, linked above.


Even the UK government now says, what some researchers and most of us anons have been saying for a while. The vaccinated CAN’T build an immune response and memory against the N protein, regardless of variant, the vaccinated body is over fixated on a dead Spike protein. Is everything starting to come together for the reader ?
At this point in time, after reading both my Reverse Marek posts, I think it is self-evident that I may be not completely right, but I am on the right track. The next 3 months will either make or break my case.
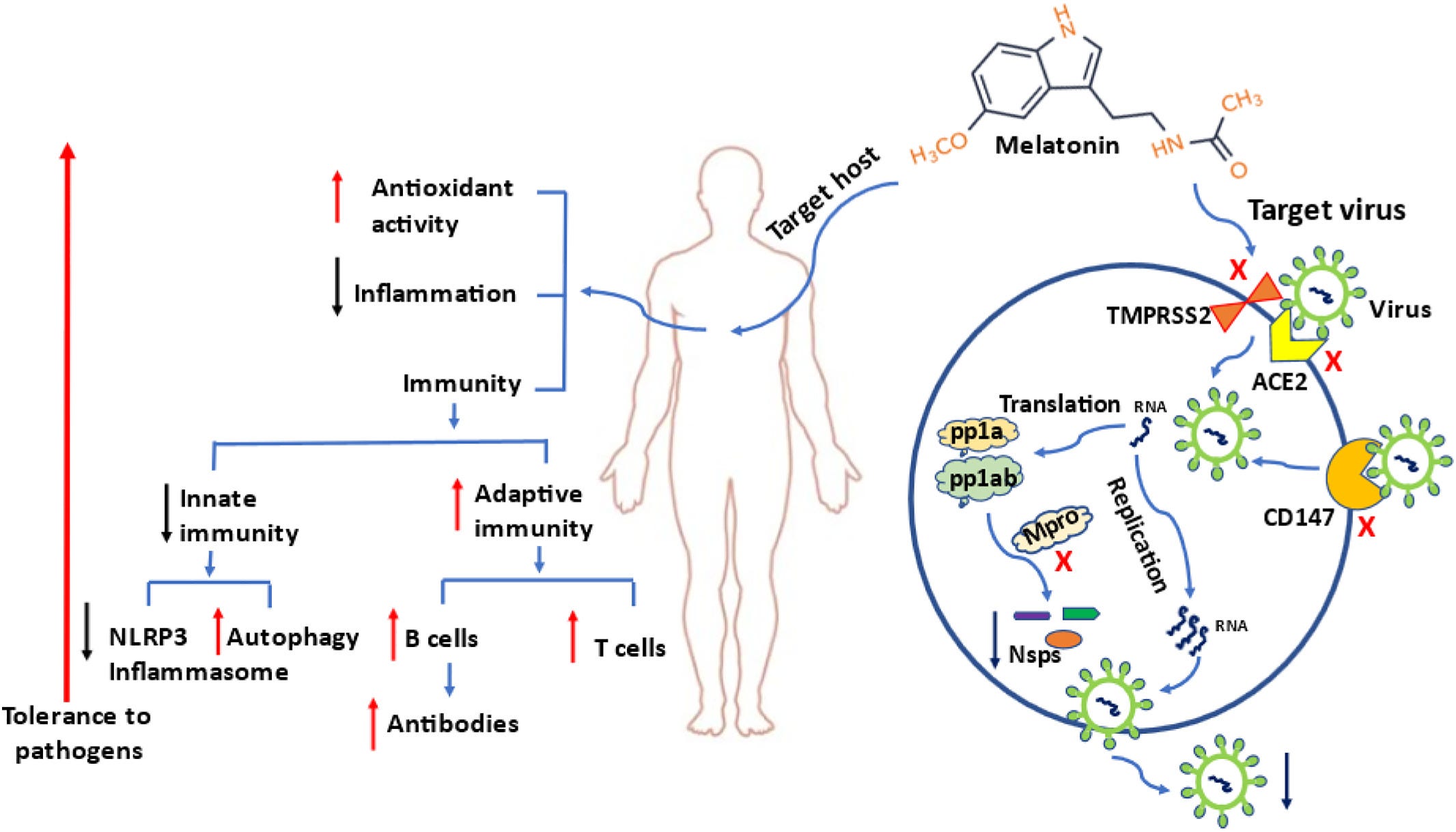
Not everything is bad news, though. This study was written by two of the world-leading Melatonin researchers and therefore experts, and they show the pathways and how Melatonin will help you deal with the infection. Not the first, but I was among them to use Melatonin to treat Covid-19 and lower mortality, given all its systemic effects and potent immunomodulatory abilities.
Mechanisms and clinical evidence to support melatonin's use in severe COVID-19 patients to lower mortality
The cost of melatonin is a small fraction of those medications approved by FDA for emergency use to treat COVID-19. Because of its self-administered, low cost and high safety margin, melatonin could be made available to every country in the world at an affordable cost. We recommend melatonin be used to treat severe COVID-19 patients with the intent of reducing mortality. If successful, it would make the SARS-CoV-2 pandemic less fearful and help to return life back to normalcy.
In March 2020 I asked why doctors were not trying to use NAC to treat patients, given all of its systemic physiological effects, especially antioxidant and anti-inflammatory.
Use of N-Acetylcysteine at high doses as an oral treatment for patients hospitalized with COVID-19
COVID-19 patients treated with NAC were older, predominantly male, and with more comorbidities such as hypertension, dyslipidemia, diabetes, and COPD when compared with those not on NAC (all p < 0.05). Despite greater baseline risk, use of NAC in COVID-19 patients was associated with significantly lower mortality (OR 0.56; 95%CI 0.47–0.67), a finding that remained significant in a multivariate analysis adjusting by baseline characteristics and concomitant use of corticosteroids.
NAC can do much more than this, and if there is ONE supplement I recommend for the vaccinated is NAC… you really need this one, but it will only make sense in part IV of the Reverse AIDS series.
If you enjoy or take value from independent interdisciplinary analysis, consider becoming a free or paying subscriber, shifting to doing it full time and with higher quality. Appreciate all supporters and new subscribers.
I love your article, especially about covid vax as a contributing factor for long covid
Official since June 29, 2021.
Levels of neutralizing antibodies CANNOT BE USED AS A SURROGATE of Spike‐specific cellular immunity induced by vaccination.
No correlation between neutralizing antibody levels and Spike-specific T cell magnitude were found.
in Rapid determination of the wide dynamic range of SARS-CoV-2 Spike T cell responses in whole blood of vaccinated and naturally infected
=>https://archive.is/r3J3N
https://www.biorxiv.org/content/10.1101/2021.06.29.450293v1.full