

Do other viruses have as many variants as SARS-CoV-2?
Finally, the changes we see in SARS-CoV-2 are also partly driven by the rapid development of vaccines and treatments designed to stop it. Compared with the early days of the pandemic, there's now much more selection pressure on the virus to escape the pharmaceutical measures designed to defeat it, Das told Live Science. Now we have multiple vaccines: antibody cocktails, convalescent plasma therapy and two drugs on the market to combat COVID. That's a lot of new pressures driving selection of the virus. Some of the mutations that stick are now the ones that will help the virus avoid these challenges.
Well, at least mainstream sources are now voicing what anon accounts have been forecasting for close to two years, and some researchers who have been ostracized by academia for close to one year. If you want to understand where this came from and where it is going, I suggest you to read “It’s viral evolution baby”, and A Case For Reverse Marek I, II and III.
A paper doing the rounds around Twitter the last two days, Autopsy Histopathologic Cardiac Findings in Two Adolescents Following the Second COVID-19 Vaccine Dose.
This post-vaccine reaction may represent an overly exuberant immune response and the myocardial injury is mediated by similar immune mechanisms as described with SARS-COV-2 and multisystem inflammatory syndrome (MIS-C) cytokine storms.38 MIS-C is a rare systemic illness presenting with persistent fever and extreme inflammation following exposure to SARS-CoV-2. Affected children have persistent fever and may have acute abdominal pain with diarrhea or vomiting, muscle pain/malaise, and hypotension. Other reported symptoms include rashes, enlarged lymph nodes, and swelling.
Conclusions.– The myocardial injury seen in these post-vaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy. Understanding that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening and therapy.
This paper sheds a lot of light in the real mechanisms of vaccine induce cardiac damage, which I always thought it was mostly immune mediated, and not purely a inflammatory response to something (usually LNP). That might be the initial trigger, but the design of the vaccine itself would be the culprit in my opinion.
Catecholamine and Catecholamine-mediated stress can induce the secretion of specific cytokines. They can shift your immune response to a Th 2 response by inhibiting IL-1, IL-2, IL-12, Interferon gamma and TNF Alpha.
Under specific conditions, it can also stimulate the production of IL-23, IL-17A and even TNF Alpha. This will be really important tomorrow. Really significant.
On the post below, I shared a paper about the mRNA being present in germinal center and lymph nodes for up to 60 days.

This will also be incredibly significant tomorrow, because you will get to understand one of the numerous pathways and mechanisms of this entire mess, just bear in mind what the paper I posted in the “Spikes Everywhere” says. Lymphs. Germinal Center. mRNA. 60 days. Expressing that specific protein for 60 days anywhere is bad, at any quantities. For now, I present the evidence, tomorrow, all else.
COVID-19 Vaccination–related Lymphadenopathy: What To Be Aware Of
With the rollout of mass COVID-19 vaccination across the world, vaccine-induced lymphadenopathy is an important side effect for clinicians, patients, and cancer researchers to be aware of.
Vaccine-induced lymphadenopathy can present as a diagnostic dilemma for radiologists.
Evolving imaging guidelines are needed to address management strategies of vaccine-induced lymphadenopathy in both the general population and high-risk oncology patients.
Documentation of vaccination status is critical to decrease unnecessary biopsies and alleviate patient anxiety.
The true incidence of postvaccination lymphadenopathy may be higher given axillary swelling was only reported as an unsolicited adverse event.
Axillary Adenopathy after COVID-19 Vaccine: No Reason to Delay Screening Mammogram
Of the 1217 patients that received the COVID-19 vaccination and had breast imaging, 537 (44%) had lymphadenopathy identified on at least one imaging exam.
Really extensive and good article about Lymphadenopathy, will write in the pertinent parts for our hypothesis.
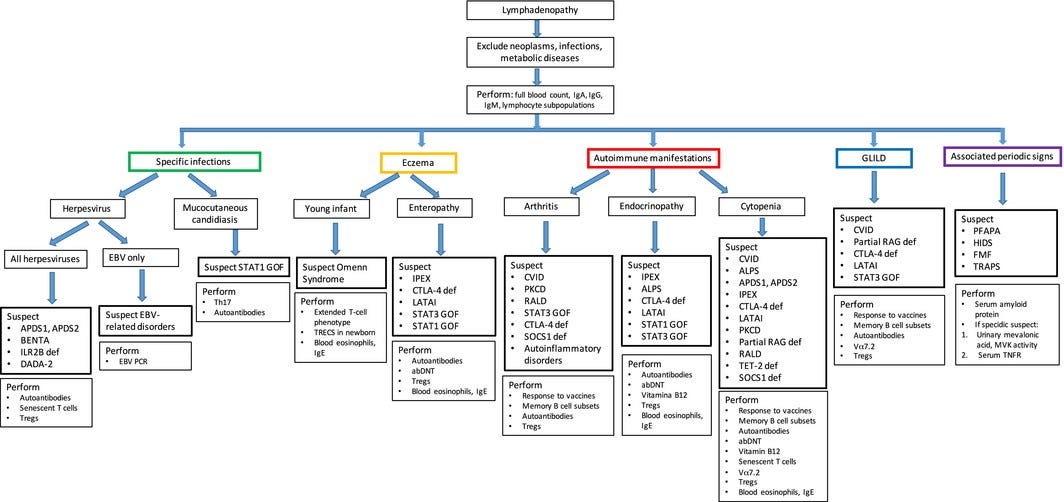
Lymphadenopathy at the crossroad between immunodeficiency and autoinflammation: An intriguing challenge
Lymphadenopathies can be part of the clinical spectrum of several primary immunodeficiencies, including diseases with immune dysregulation and autoinflammatory disorders, as the clinical expression of benign polyclonal lymphoproliferation, granulomatous disease or lymphoid malignancy. Lymphadenopathy poses a significant diagnostic dilemma when it represents the first sign of a disorder of the immune system, leading to a consequently delayed diagnosis. Additionally, the finding of lymphadenopathy in a patient with diagnosed immunodeficiency raises the question of the differential diagnosis between benign lymphoproliferation and malignancies. Lymphadenopathies are evidenced in 15–20% of the patients with common variable immunodeficiency, while in other antibody deficiencies the prevalence is lower. They are also evidenced in different combined immunodeficiency disorders, including Omenn syndrome, which presents in the first months of life. Interestingly, in the activated phosphoinositide 3-kinase delta syndrome, autoimmune lymphoproliferative syndrome, Epstein–Barr virus (EBV)-related lymphoproliferative disorders and regulatory T cell disorders, lymphadenopathy is one of the leading signs of the entire clinical picture.
Immune dysregulation syndromes
In syndromes associated with immune dysregulation, lymphadenopathies can be one of the leading signs of the clinical spectrum (Table 3). Immune dysregulation syndromes are caused by defective lymphocyte apoptosis, accumulation of self-reactive lymphocytes or altered function of regulatory T cells (Tregs) (Figure 3). A distinct subclass of immune dysregulation disorders includes diseases associated with increased susceptibility to Epstein–Barr virus (EBV)-induced lymphoproliferation.
In conclusion, due to the rarity and multi-faceted complexity of these conditions, deep critical reasoning of the clinician first observing the patient and the close collaboration with a multi-disciplinary group experienced in immunodeficiency and autoinflammation are necessary to provide an adequate diagnostic approach.