
BA. 2 and the growing case for Reverse Marek
And Bill sad about Omicron creating immunity.

First, dear old Bill is sad that Omicron fucked up their plans to population control and absolute centralization. Feels bad.

Enough memes, in to real issues. A paper doing the rounds in some circles was this one.
Virological characteristics of SARS-CoV-2 BA.2 variant
In a few months since the emergence of BA.1, we and others revealed the virological characteristics of BA.14–19. For instance, BA.1 is highly resistant to the vaccine-induced humoral immunity and antiviral drugs4–11, 16–19. Also, the spike (S) protein of BA.1 is less efficiently cleaved by furin and less fusogenic than those of Delta and an ancestral SARS-CoV-2 belonging to the B.1.1 lineage11, 12. Further, the pathogenicity of BA.1 is attenuated when compared to Delta and an ancestral B.1.1 virus12–14. However, the virological characteristics of BA.2 remains unaddressed.
Similar to BA.1, BA.2 was also highly resistant to the vaccine-induced antisera. Also, BA.2 was almost completely resistant to two therapeutic monoclonal antibodies, Casirivimab and Imdevimab, and was 35-fold more resistant to another therapeutic antibody, Sotrovimab, when compared to the ancestral D614G-bearing B.1.1 virus
These data suggest that BA.2 is more rapidly and efficiently spread in the lung tissues than BA.1.
Here, we elucidated the virological characteristics of BA.2, such as its higher effective reproduction number, higher fusogenicity, higher pathogenicity when compared to BA.1. Moreover, we demonstrated that BA.2 is resistant to the BA.1-induced humoral immunity. Our data indicate that BA.2 is virologically different from BA.1 and raise a proposal that BA.2 should be given a letter of the Greek alphabet and be distinguished from BA.1, a commonly recognized Omicron variant.
However, BA.2 S exhibited higher fusogenicity than BA.1 S without the increase of S cleavage efficacy. In recent studies12, 23, we have proposed that the fusogenicity of SARS-CoV-2 variant is closely related to its pathogenicity. This hypothesis is further supported by the observations in BA.2 in the present study. However, unlike Delta, the higher fusogenicity of BA.2 appears to be not attributed to the higher efficacy of S cleavage11, 12, 23, 27. Moreover, although TMPRSS2 increased the efficacies of both cell-cell fusion23 and cell-free infection mediated by B.1.1 S and Delta S, TMPRSS2 increased the efficacy of BA.2 S-mediated cell-cell fusion but did not affect that of BA.2 S-mediated cell-free infection. These observations suggest that TMPRSS2 contributes to the cell-cell fusion and cell-free infection mediated by BA.2 S with different mechanisms of action.
Third, it would be most critical for global health that BA.2 exhibits higher pathogenicity than BA.1
So this paper making the rounds. As I previously wrote in some of my virus posts, it is no surprise Omicron, and its new offspring, BA.2 developed quite a strong resistance toward vaccine-elicited immunity, as other papers showed, and to monoclonals.
What is concerning is that BA.2 now can get into the lungs, something that BA.1 didn’t do, and was praised as a Live Attenuated Vaccine for.
BA.2 replicate faster, it’s more pathogenic, more fusogenic (it creates more cellular mess that hinders your ability to fight infections), and I expect it to be more immunosuppressive too, but this one will take months to research, if they do it. It also passes through BA.1 immunity, so it now has more immune evasive properties (as per the first paragraph).
It is something to keep an eye out, for and focus research on, especially under the immuno-compromised scenarios. What is fairly interesting is the following, there is very little evidence of pathogenicity of BA.2 in Africa, yet there is a perceptible one in highly vaccinated countries like Denmark,
If the new subscribers read most of my virus posts (start with this one, A case for Reverse Marek) this isn’t something new, it has been my argument for a few weeks. The vaccinated are experiencing varying degrees of ADE. Vaccine enhancement of viral disease. Or what I call Reverse Marek.
Keep an eye out for any country where BA.2 dominates, and its death numbers, sadly, this will be hard to track, because the last country that was honest with the data, decided not to anymore. Nothing much to add besides reading my other virus posts.
In Spikes Everywhere, besides other problems about the S Protein, I shared a paper where they found mRNA from the vaccine up to 50 days in Germinal Centers. And, here we go.
Early approval of COVID-19 vaccines: Pros and cons
An mRNA vaccine has no risk of genomic integration, but there are several limitations. The length of antigen expression can last for several months in the case of both DNA and RNA vaccines. In general, mRNA/DNA vaccines serve as a constant long-term antigen production factory, which may not equate with successful immune responses and may even damage the expected immune effect and contribute to T cell exhaustion.51–53 However, the current mRNA vaccines might be the safer and cleaner than conventional vaccine technologies since mRNA is translated then quickly degrades, leaving nothing behind except vaccine-induced neutralizing antibodies. In contrast, in next-generation mRNA vaccines, the self-amplifying mRNA encodes not only the antigen but also the viral replication machinery leading to high levels of antigen expression, which may provide longer stimulation, hence a long-lasting duration of protection.
Supposedly the mRNA quickly degrades… so what happens when there are still mRNA in Germinal Centers for up to 50 days, with probably antigen presentation, therefore some amount of immune elicitation?
Another prominent issue might be that certain nucleic acid-based vaccines elicit strong type I interferon responses that have been related to inflammation potentially leading to the development of autoimmune disease.54–56 Epitope spreading and bystander activation, as well as autoinflammatory dysregulation in genetically prone individuals, can also lead to acute and chronic autoimmunity throughout and after COVID-19 vaccination.57,58
Vaccine-associated enhanced disease (VAED) is very rare but tends to cause serious adverse infection outcomes relative to infection without previous vaccination. VAED is also known as antibody-dependent enhancement (ADE), a disease in which secondary infection is directly facilitated by pathogen-specific antibodies produced by vaccination or primary infection
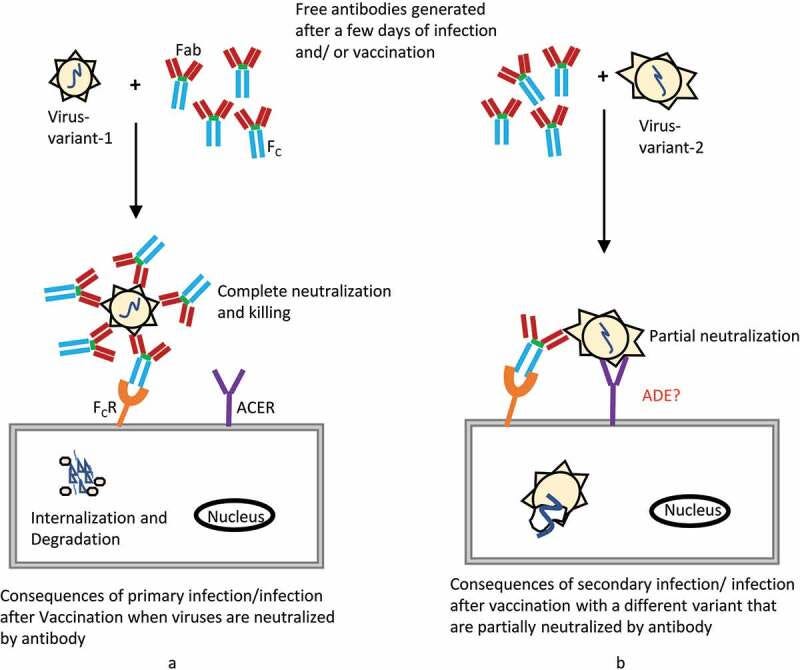
In the context of COVID-19 vaccine production, one of the possible risks posed is whether the immune responses elicited by the vaccine may boost the acquisition of SARS-CoV-2 or make the disease worse during reinfection or when infection occurs after vaccination.
I missed this entire paper when it got published, which is a shame. Read this entire post “A Case for Reverse Marek”, tell me if you can pinpoint or correlate that paper and my post.
4th Dose COVID mRNA Vaccines’ Immunogenicity & Efficacy Against Omicron VOC
Breakthrough infections were common, mostly very mild, yet, with high viral loads. Vaccine efficacy against infection was 30% (95%CI:-9% to 55%) and 11% (95%CI:-43% to +43%) for BNT162b2 and mRNA1273, respectively. Local and systemic adverse reactions were reported in 80% and 40%, respectively.
Breakthrough cases were defined only from day 8 (in each arm as well as in the control group), to exclude early infections due to exposure before vaccine is effective. All breakthrough cases were assessed by electronic questionnaires or telephone calls to define symptom severity at the end of their infection period.
The proportion of responders increased from 61% to 87% and the average IFNγ activated T cells increased from 72±13 to 203±36
Yet, most of these infected HCW were potentially infectious, with relatively high viral loads.
A new paper doing the rounds today, Saturday, and while people are paying attention to the absolutely ridiculous efficacy, which we all knew it was borderline shit, two points stood out.
First, a point that I consistently brought up and wrote an entire article about is Reverse AIDS Part III, which my point being the vaccine stimulates IFN gamma too much, leading to specific immune differentiation, and possible nasty adverse effects.
And the second point, which I have many times, is we are living in a Reverse Marek scenario. The design of the paper itself (counting as vaccinated only after day 8) is a huge signal that they are ignoring, the now well-documented, immune suppression after vaccination. Nothing further to add besides the reader referencing the posts I linked and reading them again, just cataloging further evidence for my hypothesis… and the damage to follow.
If BA.2 dominates the super vaccinated nation, given what we know, even if BA.2 has a different cytokine profile than other variants, as BA.1 seems to possess, I don’t think the vaccinated population will be able to withstand it for long. Time to remind the reader, that any vaccinated individual with only the Spike protein can never develop full immunity against the virus, they have poor N protein responses.
Scientists pinpoint mechanisms associated with severe COVID-19 blood clotting
group of researchers, including those who work at the National Institutes of Health, identified “rogue antibodies” that correlate with severe illness and may help explain mechanisms associated with severe blood clotting. The researchers found circulating antiphospholipid antibodies, which can be more common among people with autoimmune disorders, such as lupus. However, these “autoantibodies,” which target a person’s own organs and systems, can also be activated in response to viral infections and activate other immune responses.
Nothing new here, APS (Antiphospholipid syndrome) has been widely documented in both SARS-CoV-2 infection, and vaccination, a few of the reasons are below.

Another aspect of this is the endothelial dysfunction caused by both infection, platelet dysfunction (sCD40l) , and guess…
Th1/Th2/Th17/Treg expression in cultured PBMCs with antiphospholipid antibodies
The aim of this study was to evaluate the expression of T-helper cell subtypes Th1, Th2, Th17 and Treg in antiphospholipid syndrome (APS), and whether they are related to anti-cardiolipin antibody (aPL) titers. Peripheral mononuclear cells (PBMCs) were isolated from healthy donors, and incubated with aPLs. Subsequent to a 48‑h incubation, PBMCs were collected and detected by flow cytometry. The results revealed that aPLs at higher concentrations may induce a significant increase in Th2 and Th17 frequencies, as opposed to a significant decrease in Th1 and Treg frequencies and the Th1/Th2 ratio. These results indicate that there is a Th1/Th2 imbalance, a Th17 upregulation and a Treg downregulation present in APS, and that these factors are positively correlated with aPL titers, suggesting a potential role of Th cells in the pathogenesis of APS.
If you enjoy or take value from independent interdisciplinary analysis, consider becoming a free or paying subscriber, shifting to doing it full time and with higher quality. Sharing also helps me tremendously. Appreciate all supporters.
Hi John
That's a super-interesting post.
I've recently had the BA.1 variant (just recovered) and I have NOT been vaccinated. Are you saying I am like the unvaccinated Africans who have a degree of immune protection from future viral waves (like BA.2) or not?
Was a bit confused by your statement.
It is bewildering, but we need to come to terms with the fact that the immense damage of this vax-demic, civilizationally challenging, was/is voluntary & purely man-made.
Scenes in Canada and France expose the motive and the culprits.