

The impact of SARS-CoV-2 on gestation
The impact of SARS-CoV-2 on gestation
Small analysis and a PSA

It has been a few days, first I have a PSA, mostly aimed at my supporters, but everyone else should know too. My dumb self, somehow, someway misdiluted one of my peptides, meaning I poured too little bacterostatic water inside. The usual dosage is between 250 and 500 mcg, but instead, I have been injecting north of 1000 lol, so I have been crashing a lot.
I ran my body down in the last 10 years or so, so I have a lot of damage to fix and for the first time, I am taking my recovery extremely seriously. I have completely quit my old life, which had me taking contracts that help ran my body down in between Covid infections. A problem with running peptides like this is that I become slower mentally, so you will need to bear with me. Mentally slower for a while + all low-hanging fruits being picked = longer time to write meaningful articles (and I much prefer writing meaningful/impactful rather than fillers).
In a matter of days, I already have a significant reduction in muscle fatigue and muscle pain, better cardiovascular health (this one, some ways to go), less tendon pain, and less pain overall. Physically getting stronger. And clearly there is some remyelination going on because old, forgotten reflexes are coming back. Last minute addendum is that it is also fixing my brain at an accelerated rate (brain stack + peptides will do that), and I am starting to recall memories and dreams that are very important.
Healing better than expected. I appreciate the patience of my supporters and readers alike. =)
Now to the crux of the problem. While doing a significant amount of research in 2021, both I and my mentor-friend came up with avenues that were… unsavory, to say the least. We both made a promise to not write about certain topics, and one of these was the impact Covid in any form (infection, or injection) would have on infants and kids. Enough time passed, and SARS-CoV-2 is quite literally not going anywhere, but up.
Association between situs inversus and maternal SARS-CoV-2 infection at gestational age 4–6 weeks
Context and significance
A striking increase in situs inversus cases, diagnosed by ultrasound, was observed several months following removal of zero-COVID-19 policies in China, which coincided with a surge in SARS-CoV-2 infection. The rare clinical evidence presented here reveals a previously unobserved possible fetal consequence of maternal SARS-CoV-2 infection specifically during gestational weeks 4–6. To date, visceral lateralization has never been definitively linked to a specific developmental time in humans due to the rarity of such fetal samples. This study advances our current understanding of gastrulation-stage development and possibly provides the most robust support yet linking an environmental factor to occurrence of situs inversus, opening new research directions into mechanisms of visceral lateralization in humans and consequences of SARS-CoV-2 infection in pregnancy.
Highlights
• Situs inversus is associated with SARS-CoV-2 infection at gestational weeks (GWs) 4–6
• Results herein support previously undefined visceral lateralization at GWs 4–6 in humans
• SARS-CoV-2 infection at GWs 4–6 is well supported as an environmental risk factor for situs inversus
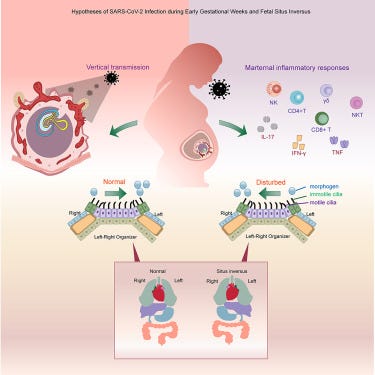
While the word sounds very complicated, situs inversus is easy to understand. You mirror, or flip the organs of a person, in very simplistic terms. Here the authors (in China) found that infection of a mother during the gestational weeks 4 to 6 can help induce sinus inversus in the fetus, and the proposed mechanisms are all well-known inflammatory proteins.
This is a rare condition, that isn’t very well understood how or why it happens, but clearly there are environmental factors such as viral infection that can predispose infants to it. While rare, you are about to read that a lot of “rare” conditions pile on top of the other when it comes to SARS-CoV-2. Such as…
The effect of long-term COVID-19 infection on maternal and fetal complications: a retrospective cohort study conducted at a single center in China
Investigate the effect of long-term COVID-19 on maternal and fetal complications. A retrospective cohort study was conducted. A total of 623 pregnant women who delivered in Kunming First People's Hospital from November 1, 2022 to July 31, 2023 were selected. By employing statistical methods, we compared the associations between maternal and fetal complications in pregnant women with acute COVID-19 during pregnancy, long-term COVID-19, and non-COVID-19 pregnant women. In the final 623 samples, there were 209 pregnant women with acute COVID-19, 72 pregnant women with long-term COVID-19, and 342 pregnant women without COVID-19. The epidemiological and clinical characteristics of all subjects were similar. Pregnant individuals who developed long-term COVID-19 during their pregnancy had an increased risk of experiencing gestational hypertension (OR 3.344, 95% CI 1.544–7.243), gestational diabetes mellitus (OR 2.301, 95% CI 1.290–4.102), and fetal intrauterine growth restriction (OR 2.817, 95% CI 1.385–5.952). Multivariate binary logistic regression analysis showed that this association remained consistent even after adjusting for confounders and performing subgroup analyses. Other maternal and fetal complications, such as premature rupture of membranes, preterm delivery, neonatal asphyxia, and transfer of neonates to NICU, did not exhibit statistically significant associations. After linear regression analysis, the platelet count (β: − 0.127, 95% CI − 0.001–0.000) of pregnant women with long-term COVID-19 was slightly lower than that of non-COVID-19 pregnant women, and the other coagulation parameters were not statistically significant. The incidence of gestational hypertension, gestational diabetes mellitus and fetal intrauterine growth restriction in pregnant women with long-term COVID-19 is significantly increased, but it does not further increase the coagulation status.
Long-term Covid-19 is how many, if not most Chinese researchers refer to Long Covid. In the case of pregnant women who developed Long Covid symptoms during pregnancy, they had a significantly higher increase of hypertension, diabetes, and fetal intrauterine growth restriction, while coagulation status remained the same, although lower platelets than others were observed.
Long Covid on its own is already a complex nightmare, but Long Covid in pregnancy adds twice the complexity, for obvious reasons. Still, the previous articles also give us necessary insights into how potentially Covid could be causing these other changes in gestating mothers.
Preeclampsia (PE) is characterized by new onset hypertension (HTN), intrauterine growth restriction (IUGR), multi-organ dysfunction, and is associated with increased inflammatory cytokines, such as interleukin 17 (IL-17).
A similar immune response, often a byproduct of immune dysregulation is one of the main pathways that causes these depressing changes in gestating mothers and their infants.
SARS-CoV-2 replicates in the placenta after maternal infection during pregnancy. Could SARS-CoV-2 replicate in the placenta (thus explaining how the virus bridges a lot of defenses and causes these negative changes) ?
SARS-CoV-2 replicates in the placenta after maternal infection during pregnancy
Conclusion: We report evidence of active in vivo SARS-CoV-2 replication in the placenta after maternal infection in pregnancy in a case–control setting in a large population. Intensity of placental viral replication as well as viral levels were higher in women with severe or critical COVID-19 disease, supporting the rationale that severity of maternal SARS-CoV-2 infection could correlate with the severity of placentitis. Replication was maximal in cases of stillbirth, which suggests direct placental involvement in the pathophysiology of this dramatic outcome. Continuing to advocate for preventive measures against COVID-19 during pregnancy, including (re)vaccination, as well as appropriately counseling women with diagnosed infection, are of utter importance.
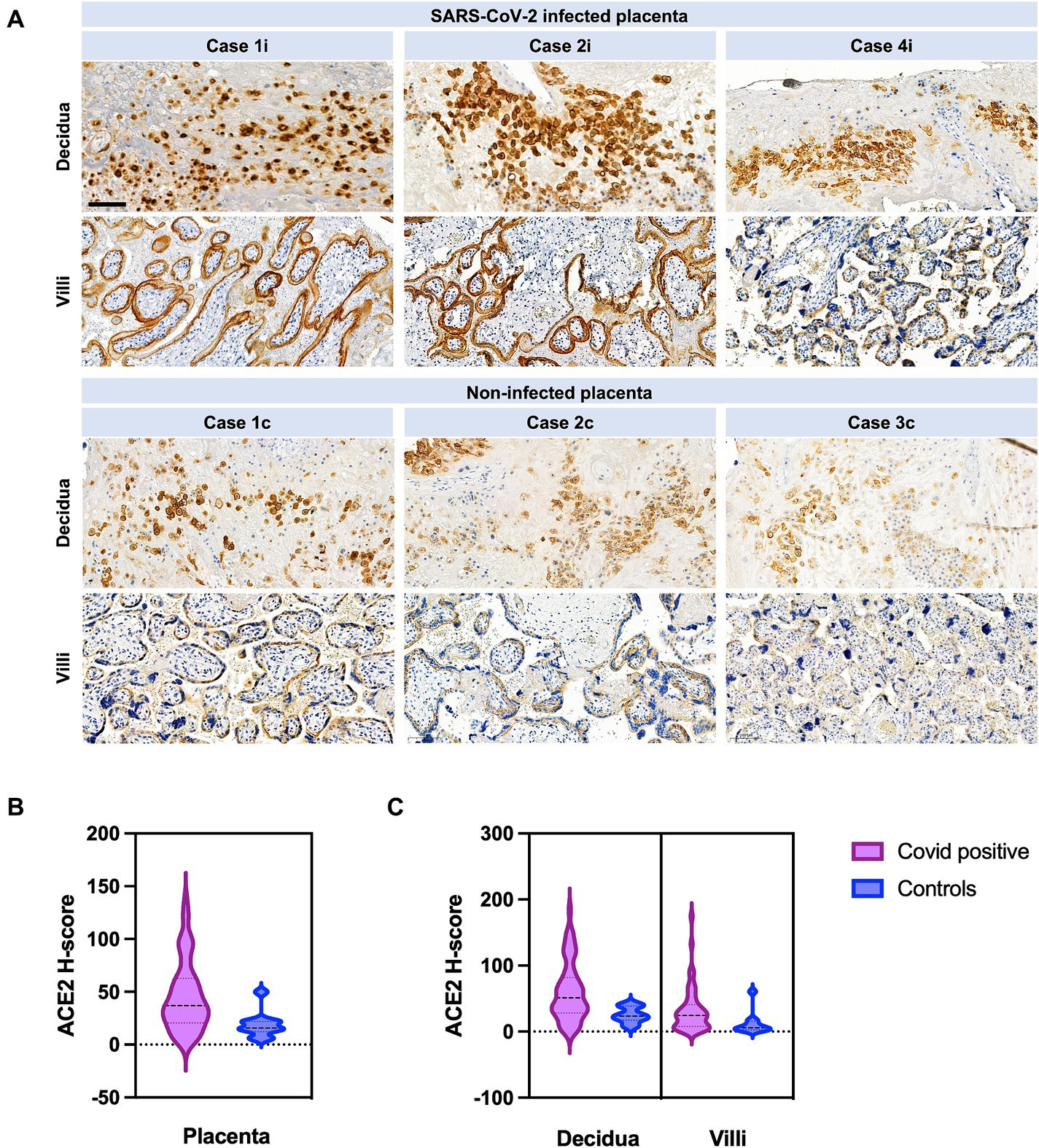
This study was done during the now very infamous, well-known “Delta wave”, arguably the worst Covid wave, perhaps only to be displaced by Wuhan wave, providing insight into how virulent and aggressive that strain was. While the rate of replication varied, 5% intense, low to moderate 20% of placentas from women infected with Covid.
The higher the replication rate, the higher the chances for stillbirth, the most drastic outcome of maternal infection with SARS-CoV-2, and while the authors avoid proposing placental infection causes the changes discussed here, I will. They can’t propose without proper evidence, but the signs are there, productive infection of the mother tissues, and placenta, leads to a flood of inflammatory response, and changes in receptors, thus leading to more changes in the fetus.
Before going to the last one, which will be significant in so many ways in the future, I need to bring to your attention one specific case reported in the paper above. “Case2i massive proliferation of the intervillous fibrin with single intercalated lymphocytes and macrophages”. The second case reported here had extensive deposition of fibrin in the placenta.
You can search for any of the conditions discussed here adding HMGB1, and you will be surprised (or not), that higher levels of HMGB1 are responsible or have a significant role in these conditions and gestational complications. Also, almost 2 years ago I found this paper and wrote about it, and you should revisit it. HMGB1 is what allows Spike and the virus to penetrate bone marrow.

Mild/Asymptomatic Maternal SARS-CoV-2 Infection Leads to Immune Paralysis in Fetal Circulation and Immune Dysregulation in Fetal-Placental Tissues
In the placental paper above, the drastic outcomes to the fetus came from infection severity, which to me isn’t the correct argument for most effects related to this chimera. This is a somewhat old paper that I read multiple times but didn’t write about for reasons cited at the start. The author states there is no “vertical transmission”, from mother to child in this study.
This paper is incredibly complex and deserves to be broken down again within a broader…septic context. Here the authors analyzed the umbilical cord blood (UCB). The cord blood and placental tissues were collected at delivery from newborns of mothers with mild or asymptomatic infection at delivery time, and of course, there were controls with no infection.
SARS-CoV-2 infection altered the levels of many immune markers in cord blood, both innate immune cells and lymphocytes (CXCL8, 9, 10, CCL4, 3, 11 CXCL11), several antiviral and pro-inflammatory mediators, notably IFNβ, TNFα, IL-23 (Th17), and IL-15 (NK cell activation), were also lower. Lymphocyte survival factors were also lower. S100B, a marker for CNS injury was increased. This means systemic inflammation with a skewed immune response.
Alongside these changes, markers of anti-inflammatory regulation such as IL-1RA were increased, showing a shift into an immuno-regulatory state. This imbalance between activation and suppression mirrors patterns seen in other severe immunological conditions, like sepsis-induced immune paralysis, where the immune system fails to respond effectively to infections despite being primed for action.
Further analyzing the blood, and the many different immune cell groups, such as B, T cells, and non-classical the authors uncovered a state of what can be called “immune paralysis”, this is a paradoxical state where the body has a higher inflammatory response but it mounts a weaker immune response when it encounters a pathogen.
The developmental origins of health and disease (DOHaD) hypothesis suggests that prenatal exposures, such as maternal infections, can program long-term susceptibility to diseases. The immune dysregulation here, particularly the imbalance in CD4+ T cells, CD8+ T cells, and monocytes raises concerns about the potential for increased vulnerability to infections or autoimmune diseases in children later in life. The observed decrease in chemokines like CXCL9, CXCL10, and CCL4, which are critical for recruiting immune cells, suggests a compromised ability to respond to infections postnatally.
A significant and profound change in how newborn cells respond to different pathogens, viral and bacterial was observed and this does dictate a lot of longer-term health outcomes, for example, responses more strongly to E.Coli LPS, and significantly weaker to RSV stimulation.
In regards to this paper, this is something I have proposed before and will propose to start working on an encompassing hypothesis in this regard. You can go on Google News and search for “sepsis” and you get a deluge of adult, and especially adolescent and child cases, all tragic. My proposition is that the Spike, whichever form you get, induces a state of immune paralysis that can last weeks (10+ weeks). And then you get infected, and things change, and your immune cells tank or fluctuate. Rinse, repeat.
If you can “stomach” looking into the morbidity that is the effects of mRNA in gestants and fetuses, I left hints in the “Welcome to the SuperFamily” article, you just need to research what each of the genes upregulated by JAK-STAT after Interleukin-12 stimulation does.
There is a small chance I go for a short hike this weekend, so I will try to get more done and publish articles in this simpler style.
As usual, I appreciate your support because that is what enabled me to start fixing myself.

I wanted to thank you for teaching me the importance of learning to rely on myself. Reading your posts over the years, that’s the message I received.
Like any dedicated caregiver, writer, researcher, or anyone who gives so much to others, there comes a point when you must remember that your own well-being is just as important as those you care for.
You've shown that taking the time to heal yourself while continuing to produce quality work is not easy, but if anyone can manage it with grace, it's you.
You have spent much of your adult life giving to others in one way or another. You've tried to educate people about the harm that COVID can cause, yet many still resist truly hearing the message, even after it impacted you. Rather than acknowledging the reality, some will continue searching for alternate explanations, missing the core truth. Even as you say, I am for the first time actually taking time to heal. I will never understand it. Your ability to heal from this will, in turn, help others heal as well. I have no doubt.
It’s a tough article to read because the truth can be hard to face, but it's necessary. I'll need to read it a few more times to fully grasp what’s happening to these sweet, precious babies.
I prefer quality over quantity. Truth over fiction.
Pfizer Covid19 Jab tests performed by Charles River found 2 Wistar Rat pups had Situs Inversus.
This and related conditions Kartagener Syndrome, Primary ciliary dyskinesia 2 and Dextrocardia are associated with Endotoxin at the US CTD.
https://geoffpain.substack.com/p/endotoxin-harms-list-l-z